
This sample Communities That Care Research Paper is published foreducational and informational purposes only. If you need help writing yourassignment, please use our research paper writing service and buy a paper on any topic ataffordable price. Also check our tips on how to write a research paper, see the lists of criminal justice research paper topics, and browse research paper examples.
Communities That Care (CTC) is a community-based operating system for decreasing risk, enhancing protection, and reducing problem behavior in youth community wide. The approach has been developed and modified through community input and formative evaluation over 20 years. CTC provides communities with a structure for engaging stakeholders to improve youth development; a process for establishing a shared community vision; tools for assessing levels of risk and protection experienced by community youth; and a framework for prioritizing risk and protective factors, implementing evidence-based programs to address them, and monitoring and assessing attainment of specific, measurable community goals. CTC has been implemented in over 500 communities across the United States and countries including Australia, Canada, Croatia, Germany, the Netherlands, and the United Kingdom. All materials needed to implement CTC can be downloaded from http://www. communitiesthatcare.net. CTC has been found effective in reducing youth delinquency, violence, and tobacco and alcohol use in the Community Youth Development Study (CYDS), a randomized controlled trial conducted in 24 communities in seven states across the United States. This research paper describes the theory underlying CTC, key features of successful community mobilization efforts, the five phases of CTC implementation, system-and youth-level findings from the CYDS, implementation challenges, and steps to broader dissemination.
Foundation
Over the past 35 years, prevention science has emerged as a discipline built on the integration of life course development research, community epidemiology, and preventive intervention trials. Researchers have identified longitudinal predictors, like family conflict or early academic failure, that increase the likelihood that young people will engage in problem behaviors associated with significant morbidity, and in some cases, mortality (Catalano et al. 2011; Hawkins et al. 1992b; Patton et al. 2009). Other predictors, like strong bonds to positive adults or the development of specific competencies, are protective, associated with reducing problem behaviors and increasing favorable outcomes like academic success, even in the presence of risk (Catalano et al. 2011). Many risk and protective factors are predictive of multiple adolescent problem behaviors, suggesting that improvements can affect a broad set of outcomes simultaneously.
Researchers have designed interventions to reduce risk and enhance protection and in controlled trials have found a number of preventive interventions to be effective in reducing prevalent and costly problems, including adolescent substance use and delinquency. There is a growing evidence base of what works to prevent youth problem behaviors and promote healthy development, and several lists of tested and effective programs have been made available to the public (see, for example, the list of programs identified at www.colorado.edu/cspv/blueprints, www.cochrane.org, and www.campbellcollaboration.org).
In spite of these advances, tested and effective approaches to preventing youth problem behaviors have not been widely adopted (Ringwalt et al. 2009). Reasons include a lack of knowledge about scientifically proven prevention programs, difficulty marshaling resources for science-based prevention and health promotion efforts, and failure to implement proven programs with fidelity. The Communities That Care (CTC) prevention system, which mobilizes community stakeholders to collaborate on the implementation of a science-based community prevention system, was developed to address these issues (Hawkins et al. 1992a) and has been refined over more than 20 years through community input and formative evaluation. This research paper describes the CTC approach to prevention, steps involved in implementation, major findings from a randomized controlled trial, challenges in implementing CTC, and next steps in the dissemination of CTC.
Community Mobilization Efforts To Prevent Youth Problem Behavior
Community mobilization has been promoted as a strategy for reducing risk, enhancing protection, and improving youth outcomes (David-Ferdon and Hammond 2008; Fagan et al. 2011b; Hawkins et al. 2010). Typically, at the center of these efforts are locally based coalitions composed of diverse stakeholders committed to positive youth development. Community mobilization is promising because of coalitions’ intimate connections to and knowledge of the local environment, capacity for sharing information and resources among service providers and others, and potential to efficiently provide prevention services in an organized manner and without duplication. Coalition responsibilities often focus on planning and coordinating prevention activities, which may involve implementing specific prevention programs to address local priorities, altering the environment by changing local policies and norms, or both.
In spite of their promise, community mobilization strategies have often had little success in meeting prevention goals, and many have been ineffective in reducing risk and problem behaviors (David-Ferdon and Hammond 2008; Fagan et al. 2011b; Hallfors et al. 2002; Merzel and D’Affliti 2003). Lack of success has been attributed to insufficient guidance in implementing prevention strategies, a mismatch between services and goals or inadequate service “dosage,” and failure to select and use tested and effective prevention programs and strategies (Fagan et al. 2011b). Hallfors et al. (2002) suggested that coalitions could increase their chances of success by adhering to several criteria: (a) establishing focused and manageable goals, including well-defined, measurable outcomes; (b) using evidence-based programs, receiving adequate training to carry them out effectively, and monitoring implementation with attention to both dose and quality; and (c) evaluating impact by using meaningful indicators that correspond to overall goals as well as the programs chosen. CTC’s design incorporates these recommended features.
The Communities That Care Prevention System
CTC mobilizes a broad base of community stakeholders to improve youth outcomes through the development and implementation of a science-based community prevention system. CTC “communities” are geographically defined places large enough for educational and human services to be delivered at that level. They can be incorporated towns or suburbs, or neighborhood or school catchment areas within larger cities. The community population for a CTC initiative should range from 5,000 to 50,000.
CTC is guided by thesocial development model, a theory of youth development which hypothesizes thatto develop healthy, positive behaviors, young people must be immersed infamily, school, community, and peer environments that communicate healthybeliefs and clear standards for behavior. When strong bonds exist between youthand prosocial individuals and groups, youth are more likely to adopt positivebeliefs and healthy behaviors. Bonds are fostered when youth are provided withopportunities to be actively involved in meaningful, developmentallyappropriate activities, skills to be successful in those activities, andrecognition for their efforts, achievements, and contributions to the group(Catalano and Hawkins 1996). In addition to supporting the implementation ofevidence-based prevention practices that reduce risk and enhance protectivefactors, CTC encourages community stakeholders to adopt the social developmentmodel in their daily interactions with young people and ensure that they areprovided developmentally appropriate opportunities, skills, and recognition, aswell as healthy standards for behavior. The social development model alsounderlies CTC community mobilization and training efforts. CTC createsopportunities for all interested stakeholders to participate in developing ashared vision for positive youth development based in prevention science. Diverse community representatives develop skills to work together effectivelyand are recognized for their efforts and contributions to youth development.Social bonds among coalition members enhance their commitment to science-based prevention work.
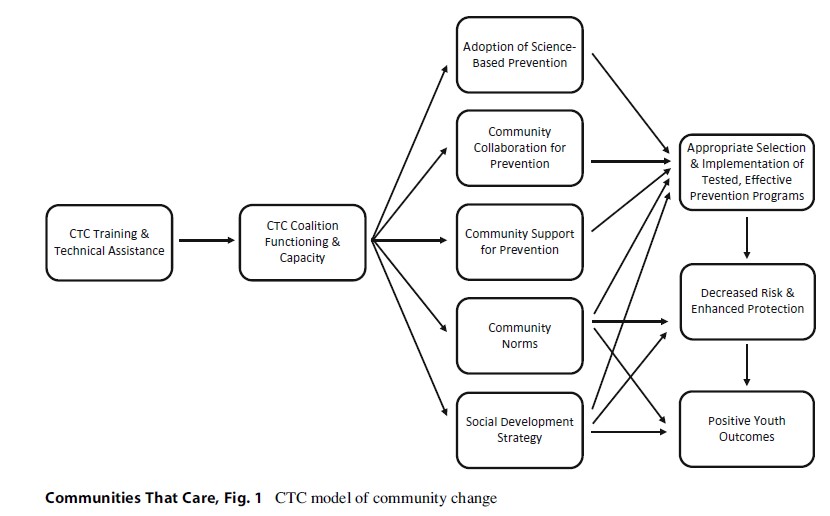
CTC’s theory of changeis depicted in Fig. 1. Training and technical assistance by certified CTC trainers serves as a catalyst for the development of the community preventionboard, which commits to using a risk- and protection-focused approach topreventing youth problem behaviors. The coalition utilizes survey data toidentify elevated risk factors and depressed protective factors within thecommunity and then prioritizes which to address through evidence-basedprevention programs targeting their priorities. The coalition facilitates broaderprevention service system transformation by encouraging collaboration and theadoption and faithful implementation of tested and effective preventionprograms aimed at prevention goals. Community prevention actions are expectedto lead to reductions in risk and enhancements in protective factors, which inturn are expected to lead to more positive youth outcomes. Community-levelimpacts on risk and protective factors are expected 2–5 years followingfaithful implementation of tested and effective programs, and community-widechanges in youth outcomes are expected to occur within 4–10 years.
CTC Implementation: Providing Communities With The Tools, Skills, And Knowledge To Achieve Local Prevention Priorities
A major challenge for prevention scientists committed to applying research in the “real world” is increasing the use of tested and effective prevention practices while recognizing that communities differ from one another and need to decide locally what effective policies and programs to use. Local control is built into CTC from the beginning. CTC provides education and tools to build community capacity for using prevention science to decide which risk and protective factors and outcomes to prioritize and which tested and effective programs and policies to implement to address community-specific concerns. It takes communities approximately 1 year to complete CTC’s five training phases and develop the skills and knowledge to choose and faithfully implement evidence-based prevention programs addressing local priorities (Hawkins et al. 2008b; Quinby et al. 2008). Each phase has specific milestones and benchmarks and includes training and technical assistance provided by a certified CTC trainer.
Phase 1: Get Started. In this phase, community leaders concerned with preventing youth problem behaviors assess community readiness to adopt the CTC system, as well as any barriers to implementation. Readiness requires collaboration among multiple stakeholders and a shared belief that reducing risk and improving protection can prevent problem behaviors. Community stakeholders need to be willing to establish shared goals and collaborate to achieve them. If these attitudes are not present, community readiness needs to be improved before implementing CTC. Other major activities include identifying one or two key leaders to champion CTC, hiring a coordinator to manage CTC activities, and obtaining school district support for conducting a youth survey that will provide local epidemiological data on risk, protection, and youth behaviors.
Phase 2: Organize, Introduce, and Involve. The major task in Phase 2 is to identify and train two key groups from the community in the principles of prevention science and the CTC prevention system. The first group consists of key community leaders and influential stakeholders (the mayor, police chief, school superintendent, and business, faith, community, health, social service, and media leaders) who are introduced to CTC during a half-day Key Leader Orientation that includes information about prevention science and the relationship between youth risk and protective factors and problem behaviors. Key leaders are responsible for securing resources for preventive interventions identified through the CTC process and identifying candidates for the CTC Community Board, a demographically diverse and broad-based coalition charged with carrying out CTC planning and prevention activities. The second group, the Community Prevention Board, participates in a 2-day Community Board Orientation. The board develops a vision statement to guide its prevention work and establishes workgroups to perform core implementation and maintenance activities: board maintenance, risk and protective factor assessment, resource assessment and analysis, public relations, youth involvement, and funding.
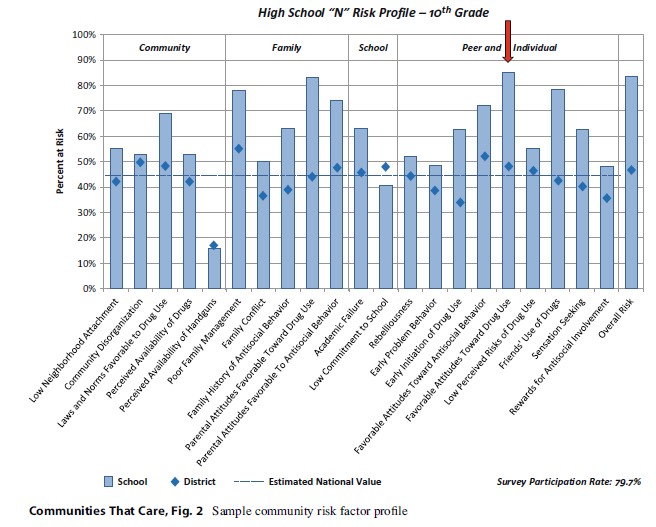
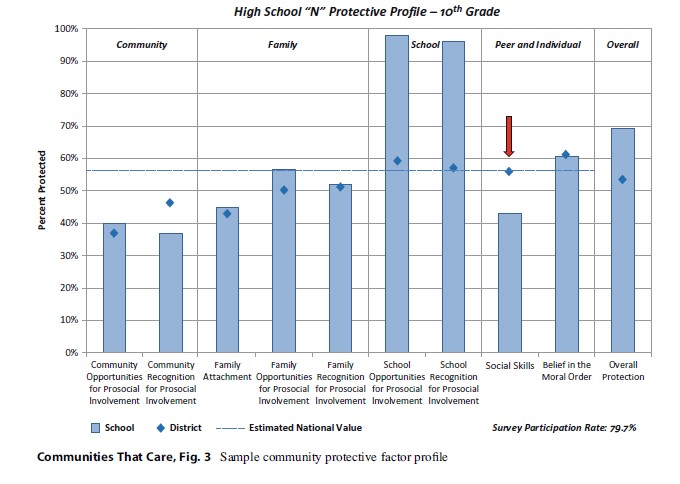
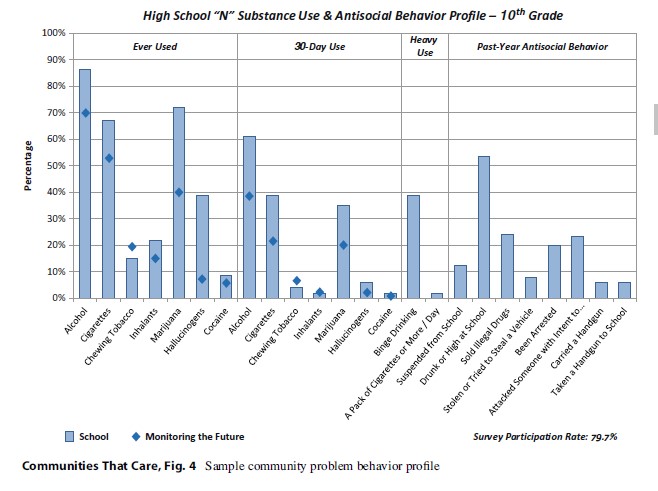
Phase 3: Develop a Community Profile. In Phase 3, the CTC board develops a community profile of risk, protection, and problem behavior among community youth; targets two to five risk and protective factors for preventive action; and identifies existing prevention resources and gaps. The first two activities are accomplished in a 2-day Community Assessment Training. The major source of data for the community profile is the CTC Youth Survey (Arthur et al. 2007), a school-based self-report questionnaire administered to students in Grades 6, 8, 10, and 12 that measures risk and protective factors experienced by young people, as well as their involvement in problem behaviors like substance use, delinquency, and violence. These data are summarized in a community profile, like the one shown in Figs. 2, 3, and 4. Each profile is unique to the community. Among 10th-grade students in the alternative high school depicted in Fig. 2, survey data indicate a number of elevated risk factors compared to school district averages. Many are drug-related risk factors, and not surprisingly, as shown in Fig. 4, both lifetime and current drug use by 10th-grade students in this school were considerably more prevalent than among 10th graders nationally, as measured by the Monitoring the Future survey (Johnston et al. 2000). Figure 3 shows that, while a large majority of10th-grade students in this alternative school reported that the school provided many opportunities for active involvement and much recognition for student effort and achievement, many fewer students had strong social skills, including skills to avoid or refuse trouble or problem behaviors. Based on these data, this community’s CTC board chose to reduce the risk factor “favorable attitudes toward drug use” and strengthen the protective factor “social skills.”
Following a CommunityResource Assessment Training, board members survey service providers whodeliver preventive intervention targeting their prioritized risk and protectivefactors to assess whether there are existing research based prevention programsalready available in the community. This ensures that any new preventionprograms chosen by the board fill existing gaps rather than duplicatingeffective prevention programs already in place in the community.
Phase 4: Create aCommunity Action Plan. In Phase 4, board members use information gathered inPhase 3 to develop a Community Action Plan. A 2-day Community Plan Trainingprovides tools and knowledge to select tested and effective programs, policies,and actions targeting priorities established in Phase 3 to fill gaps inprevention services. The board chooses programs from the CTC Prevention StrategiesGuide, a compendium of prevention programs (including parenting skills, school curricula,mentoring, after-school, and community-based programs) found effective inchanging risk, protection, and problem behaviors in at least one high-qualitycontrolled trial. The Community Action Plan specifies how the coalition willimplement the chosen prevention programs, monitor implementation quality, andassess improvement in risk, protection, and problem behaviors.
Phase 5: Implement and Evaluate the Community Action Plan. The last phase consists of implementing the Community Action Plan. The Community Plan Implementation Training emphasizes the importance of adhering faithfully to the content, dosage, and high-quality delivery specified in program protocols. Communities are directed to prevention program developers for training and technical assistance in the programs selected. Board members and program implementers learn to track implementation progress, assess changes in participants, and make adjustments to achieve program objectives. Monitoring is accomplished through the use of program-specific implementation checklists, observations, and participant pre- and posttests.
During this phase the board also engages local media to educate the community about risk and protective factor priorities and generate public support for the preventive interventions selected.
When they complete Phase 5, communities have the knowledge, tools, and skills to faithfully implement tested and effective prevention policies and programs to address locally prioritized risk, protection, and youth problem behaviors. The CTC process is ongoing. Every 2 years the CTC Youth Survey is read ministered, and resource assessment data are updated. The CTC board reviews these data to evaluate progress and revise action plans as needed. As previously noted, community-level changes in youth risk and protection are expected to occur 2–5 years after tested and effective prevention programs are implemented. Community-level effects on youth behaviors are expected 4–10 years following implementation.
The Community Youth Development Study: A Test Of Communities That Care
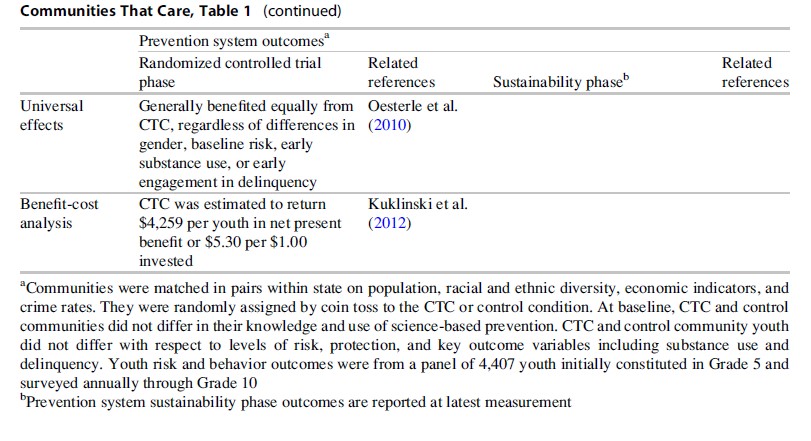
CTC has been evaluated in the Community Youth Development Study (CYDS), a multisite community-randomized trial initiated in 2003 involving 24 communities in Colorado, Illinois, Kansas, Maine, Oregon, Utah, and Washington. Participating communities are small to moderate-sized incorporated towns with their own government, education, and law enforcement structures (population range: 1,500–50,000, M ¼ 15,633, SD ¼ 10,147). Communities were matched in pairs within state on population, racial and ethnic diversity, economic indicators, and crime rates. After receiving commitments from each community’s mayor or city manager, the police chief or lead law enforcement officer, and the superintendent of schools to participate in the study, one community from each matched pair was assigned randomly to the intervention (CTC) or control condition. At the study’s start, none of the communities had advanced in the use of science-based prevention to the point of selecting and using tested, effective preventive interventions to address prioritized community risks (Brown et al. 2009; Hawkins et al. 2008b). Youth in CTC and control communities did not differ at baseline on key outcome variables including substance use and delinquency (Hawkins et al. 2008b).
To date, interventioneffects on prevention systems and youth risk and problem behaviors have beenevaluated during the intervention period and up to 20 months after interventionsupport from the study ended. Prevention system effects were evaluated based onreports of key community leaders, prevention coalition chairs, coordinators,and board members from CTC and control communities. Intervention effects onyouth risk and problem behaviors were evaluated based on reports of alongitudinal panel of 4,407 children from intervention and control communities whocompleted the CTC Youth Survey annually from Grade 5 through Grade 10. Majorintervention effects are summarized in Table 1 and are described in thefollowing sections.

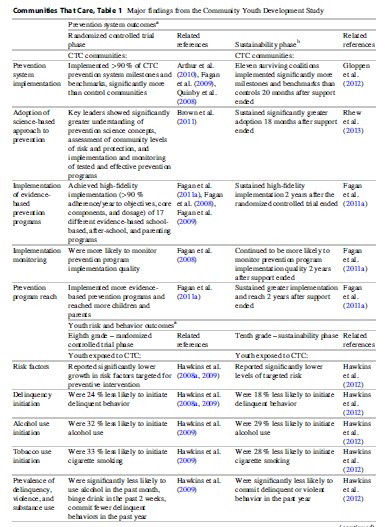
CTC Leads To Sustained Prevention System Effects
The CYDS evaluatedcommunity efforts to faithfully implement (a) the core principles of the CTCprevention system and (b) tested and effective prevention programs with respectto content and delivery specifications. Broader effects on community preventionsystems were also evaluated. CTC communities were supported by training in thefirst year and technical assistance throughout the first 5 years of the trialand achieved high implementation fidelity at the system and program levels.
High-Fidelity Implementation of the CTC Prevention System. At baseline, CTC and control communities did not differ in their use of a science-based approach to prevention (Hawkins et al. 2008b). The CTC Milestones and Benchmarks Survey was used to track progress in implementation of core components of the CTC prevention system. In each intervention year, CTC communities implemented an average of 90 % of the key features of CTC, including developing a community board, prioritizing risk and protective factors, selecting tested and effective preventive interventions from the CTC Prevention Strategies Guide, implementing selected prevention programs with fidelity, and periodically assessing risk and protective factors and child and adolescent well-being through surveys of students (Fagan et al. 2009; Quinby et al. 2008). Control communities did not make this progress over time in completing CTC milestones and benchmarks, implementing scientifically proven prevention programs, and monitoring program impacts (Arthur et al. 2010). CTC communities were able to sustain these gains 20 months after study-provided training and technical assistance ended (Gloppen et al. 2012).
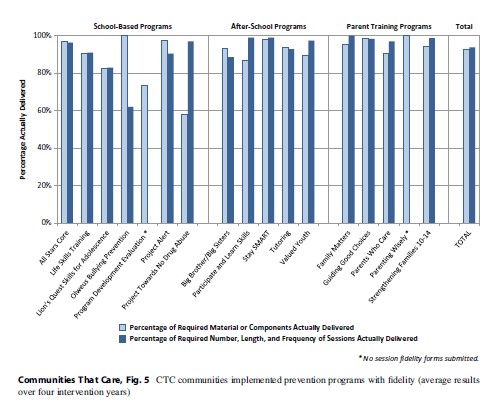
Faithful Implementationof Tested and Effective Prevention Programs. Over the course of the trial, the12 CTC communities demonstrated faithful implementation of 17 differentschool-based, after-school, and parenting interventions (shown in Fig. 5)selected from a menu of 39 possible tested and effective programs forfifth-through ninth-grade students contained in the CTC Prevention Strategies Guide(Fagan et al. 2011a, 2008, 2009). On average, CTC communities implemented 2.75tested and effective prevention programs per year (range: 1–5). High rates offidelity were achieved consistently over time with respect to adherence toprogram objectives and core components (average ¼ 91 %–94 % per year) anddosage (number, length, and frequency of intervention sessions; average ¼ 93%–95 % per year) and were sustained 2 years after CYDS support ended. Althoughcontrol communities did not implement as many tested and effective preventionprograms as CTC communities, they, too, reported implementing tested, effectiveprevention programs during the intervention and 2 years into the sustainabilityphase of the study. However, compared to CTC communities, control communitiesdid not reach as many children and parents, nor were they as likely to monitorprevention program implementation quality during the intervention andsustainability periods (Fagan et al. 2011a).
Prevention Service System Transformation. CTC’s theory of change illustrated in Fig. 1 suggests that several characteristics of the prevention service system in communities are important to achieving desired improvements in youth risk, protection, and problem behavior. By the third year of the intervention, important signs of system transformation were observed in CTC but not control communities. Key leaders in CTC communities reported a significantly higher stage of adoption of science-based prevention in their communities, meaning that they had a greater understanding of major prevention science concepts like risk and protection, and reported that their communities empirically assessed community levels of risk and protection, used tested and effective prevention practices, and monitored prevention program implementation and outcomes more than did key leaders from control communities (Brown et al. 2011). Adoption of a science-based approach to prevention is hypothesized to be a key to achieving better youth outcomes through CTC. Key leaders in CTC communities also were willing to allocate a greater percentage of funding for prevention programs than key leaders in control communities, providing some evidence of increased community support for prevention in CTC communities. Although levels of collaboration did not differ in CTC and control communities at the third year of intervention, high levels of collaboration were observed in both. Effects on adoption of a science-based approach to prevention and desired prevention funding were sustained 18 months after the intervention phase of the Community Youth Development Study ended, and, at that point, key community leaders in CTC communities reported stronger community norms against adolescent drug use than did key leaders in control communities (Rhew et al. 2013).
CTC Leads To Sustained Prevention Of Youth Risk, Delinquency, And Substance Use
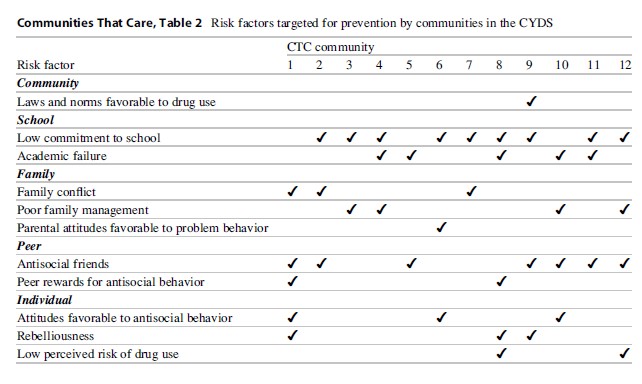
CTC communities eachprioritized 2–5 risk factors to target with tested and effective preventionprograms, as shown in Table 2. Effects on youth risk and problem behaviors werefirst observed in Grade 7, after less than 2 full years of intervention andearlier than CTC’s theory of change suggested. Effects have been sustainedthrough Grade 10, 1 year after the trial’s intervention phase ended.
Effects on Risk Factor Exposure. Longitudinal panel youth in CTC and control communities reported similar levels of targeted risk in Grade 5, when the intervention began (Hawkins et al. 2008a), but targeted risk exposure grew more slowly for youth in CTC communities between Grade 5 and Grade 10 (Hawkins et al. 2012). Significantly lower levels of targeted risk were first reported by CTC panel youth 1.67 years into the intervention, in Grade 7, (Hawkins et al. 2008a) and have been sustained in CTC panel youth reports through Grade 10.
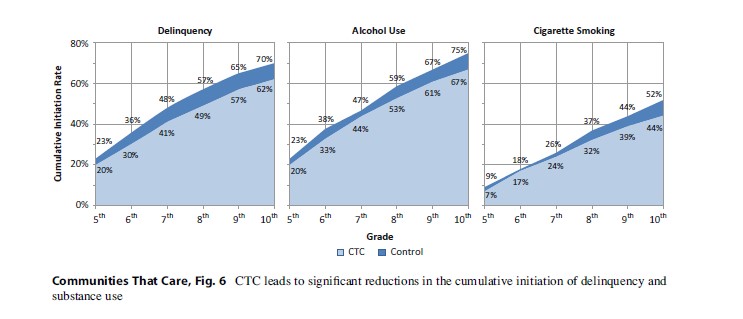
Effects on the Initiation of Delinquency and Substance Use. Panel youth from CTC and control communities also reported similar levels of delinquency, alcohol use, and cigarette smoking at Grade 5 baseline. However, between Grades 5 and 10, CTC had significant effects on the initiation of these behaviors. Significant reductions in the initiation of delinquency were first observed in the spring of Grade 7 (Hawkins et al. 2008a). Panel youth from CTC communities were 25 % less likely than panel youth from control communities to initiate delinquent behavior, and they remained 24 % less likely to do so in Grade 8 (Hawkins et al. 2009). Significantly lower delinquency initiation rates were sustained through Grade 10 (Hawkins et al. 2012), when panel youth from CTC communities were 18 % less likely to initiate delinquency than panel youth from control communities.
Preventive effects on alcohol use and cigarette use were first observed in the spring of Grade 8, 2.67 years after intervention programs were implemented. Grade 8 youth from CTC communities were 32 % less likely to initiate alcohol use and 33 % less likely to initiate cigarette smoking than Grade 8 youth from control communities (Hawkins et al. 2009). Preventive effects were sustained through Grade 10 (Hawkins et al. 2012), when CTC panel youth were 29 % less likely to initiate alcohol use and 28 % less likely to initiate cigarette smoking than panel youth from control communities.
As shown in Fig. 6,differences in the initiation of delinquency, alcohol use, and cigarettesmoking from Grade 5 through Grade 10 led to cumulatively lower rates ofinitiation over time: 62 % of 10th-grade youth in the panel from CTCcommunities had engaged in delinquent behavior compared with 70 % of 10th-gradeyouth in the panel from control communities; 67 % versus 75 % had initiatedalcohol use; and 44 % versus 52 % had smoked cigarettes.
Reductions in the Prevalence of Delinquency, Violence, and Substance Use. CTC also significantly reduced the prevalence of youth problem behaviors in Grades 8 and 10. In Grade 8, the prevalence of alcohol use in the past month, binge drinking (five or more drinks in a row) in the past 2 weeks, and the variety of delinquent behaviors committed in the past year were all significantly lower in CTC panel youth compared to control community panel youth (Hawkins et al. 2009). A subset of the delinquency items was used to create a measure of violent behavior. The CYDS found significant effects of CTC in reducing the prevalence of delinquent behavior and violence in the past year in the spring of Grade 10 (Hawkins et al. 2012). Tenth-grade students in CTC communities had 17 % lower odds of reporting any delinquent behavior in the past year (t (9) =-2.33; p =.04; AOR = .83) and 25 % lower odds of reporting any violent behavior in the past year (t (9) =02.51; p= .03; AOR = .75) compared to students in control communities.
CTC’s Effects Are Universal. CTC was designed as a universal intervention, and the universality of its effects on the prevalence of substance use and delinquent behavior was tested based on outcomes observed in panel youth in the spring of eighth grade (Oesterle et al. 2010). Four groups of students were established using baseline Grade 5 data: boys and girls, high baseline risk versus all others, early substance users versus nonusers, and early engagers in delinquency vs. non-engagers. Results generally supported the universal effectiveness of the CTC intervention with respect to the prevalence of delinquent behavior and substance use within groups. There were two exceptions. The effect of CTC on reducing the prevalence of substance use in eighth grade was stronger for boys than girls, and the effect on the prevalence of delinquency was stronger for students who were non-delinquent at baseline.
CTC Is A Cost-Beneficial Intervention
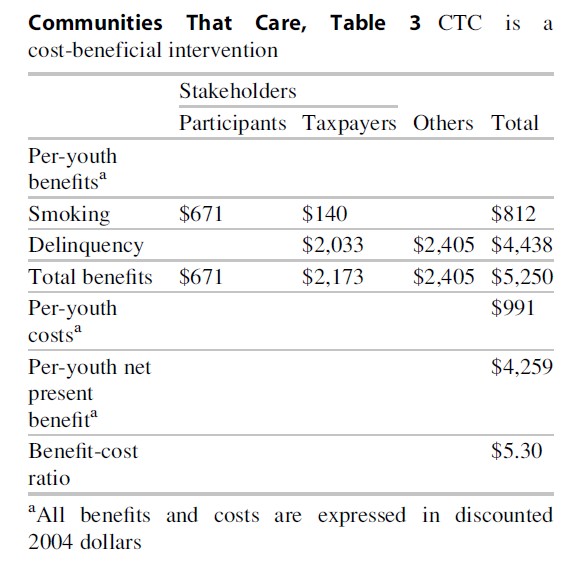
A cost-benefitanalysis was undertaken to determine whether CTC is a sound investment ofpublic dollars based on significant preventive effects on cigarette smoking anddelinquency initiation found in Grade 8 (Kuklinski et al. 2012). Findings are summarizedin Table 3. CTC’s long-term financial benefits from reduced initiation werecompared to a conservative CTC implementation cost of $991 per youth over 5years. Most communities spent significantly less, roughly $513 per youth. Approximately37 % of the total went toward a CTC coordinator and the coalition; 35 % toprevention programming; 23 % to CTC training, technical assistance, andmonitoring; and 4 % to miscellaneous expenses. Implementation costs were morethan offset by CTC’s estimated financial benefits of $5,250 per youth. Thebenefit-cost ratio indicates $5.30 is returned to society for every $1.00invested, evidence that CTC is a cost-beneficial investment.
Challenges To Implementing CTC
Like other community mobilization strategies, CTC can be challenging for communities to implement and sustain. In our experience, communities need to overcome five types of challenges to successfully own and operate CTC.
Be Ready to Implement a Comprehensive Approach to Prevention. Communities must be ready to initiate comprehensive evidence-based prevention in order to fully implement CTC. This requires readiness along several key dimensions. Differing views among stakeholders about the most effective approach to addressing youth problems must be considered. If particular groups advocate only exclusionary approaches such as arrest and incarceration, or exclusive reliance on treatment approaches, they may need further education about the potential effectiveness of prevention prior to engaging in the CTC process. If communities have an unsuccessful history of collaboration, characterized by conflict and competition for scarce resources, building trust through collaborative efforts to achieve smaller specific goals, like closing a crack house or getting a crosswalk installed on a busy street, may be necessary prior to initiating CTC.
Recruit and Engage Key Leaders. If CTC is to succeed, key community leaders who control resources and shape opinions, like the mayor, school superintendent, and police chief, must decide to bring the CTC system into their community. Their recruitment and engagement is essential to CTC’s success. Without ongoing “buy-in” from key leaders and influential champions who have access to resources, CTC will not be viable because local resources will need to be committed and often redirected to prevention.
Evidence-Based Prevention Often Competes with Usual Practice. The board needs to advocate for a risk- and protection-focused approach to preventing problem behavior and for the use of tested and effective preventive interventions to address local priorities. At times, this can mean giving up programs that are rooted in community tradition or are local favorites if they lack research evidence of effectiveness.
Faithfully Implement and Evaluate. Achieving prevention goals requires high-quality implementation of the CTC system and prevention programs and monitoring outcomes over time. Monitoring community-wide implementation and making needed adjustments can be a challenge when programs are implemented in multiple classrooms, agencies, and community settings. Evaluation of changes in risk, protection, and outcomes at the community level is also a challenge. At the local level, it may be several years before community-wide reductions are achieved, requiring long-term commitment to the CTC approach.
Ensure Adequate Resources. CTC coalitions and community coordinators represent critical human resources needed to run CTC. Maintaining board engagement and recruiting and orienting new members to CTC and the coalition’s progress to date are essential to long-term sustainability. Securing ongoing funding for coalitions and coordinators, prevention programs, and training and technical assistance can be a challenge for coalitions. In the CYDS and in a second quasiexperimental study of CTC in Pennsylvania (Feinberg et al. 2008), coalitions were aided in initial implementation efforts by seed money for coalition organizing and training and implementing chosen effective prevention approaches. Many coalitions in both studies have demonstrated success in generating ongoing resources for CTC. Those most likely to obtain funding were well functioning and planned for financial sustainability as part of their regular operations (Feinberg et al. 2008).
Steps To Broader Dissemination Of CTC
All manuals and materials needed to implement CTC have been placed in the public domain by the US Substance Abuse and Mental Health Services Administration of the Department of Health and Human Services and are freely available at http://www.communitiesthatcare.net. CTC is currently being implemented in communities across the United States and in countries including Australia, Canada, Croatia, Germany, the Netherlands, and the United Kingdom. The CTC tests in both the Community Youth Development Study and the Pennsylvania quasi-experimental study were conducted with certified providers of training and technical assistance, as well as monitoring and oversight of implementation, including reviewing and providing feedback on annual plans. State and federal governments, local philanthropic organizations, the United Way, and other local funders could assist in broader dissemination of CTC by supporting training, technical assistance, and monitoring of processes and outcomes. Efficiencies can be achieved by offering CTC training through state governments, who can then train state prevention workers and contractors to deliver CTC training and technical assistance to local communities. A national CTC training and certification center could support the training of state and community personnel in CTC and share lessons learned from the implementation of CTC.
Conclusion
Policymakers and researchers increasingly recognize the need for clear and compelling evidence about how best to prevent prevalent and costly problem behaviors in youth. Delinquency and substance abuse are problems that begin in late childhood and adolescence, often with lifelong consequences. The results of the Community Youth Development Study show that Communities That Care, a coalition-based prevention system employing a riskand protection-focused approach, is a cost-beneficial, effective way to prevent delinquency, violence, and tobacco and alcohol use in youth. Intervention communities were able to faithfully implement the CTC prevention system and evidence-based programs designed to address community-specific prevention priorities, and they sustained this success after the intervention phase of the Community Youth Development Study was over. These efforts were related to significant, meaningful, and sustained reductions community wide in the percentage of youth in intervention communities initiating delinquent behavior, alcohol use, and cigarette smoking, and in the prevalence of current involvement in smoking, delinquency, and violence when compared to youth from control communities.
Bibliography:
- Arthur MW, Briney JS, Hawkins JD, Abbott RD, BrookeWeiss BL, Catalano RF (2007) Measuring risk and protection in communities using the Communities That Care Youth Survey. Eval Program Plann 30:197–211
- Arthur MW, Hawkins JD, Brown EC, Briney JS, Oesterle S, Abbott RD (2010) Implementation of the Communities That Care prevention system by coalitions in the Community Youth Development Study. J Community Psychol 38:245–258
- Brown EC, Graham JW, Hawkins JD, Arthur MW, Baldwin MM, Oesterle S, Briney JS, Catalano RF, Abbott RD (2009) Design and analysis of the Community Youth Development study longitudinal cohort sample. Eval Rev 33:311–334
- Brown EC, Hawkins JD, Arthur MW, Briney JS, Fagan AA (2011) Prevention service system transformation using Communities That Care. J Community Psychol 39:183–201
- Catalano RF, Hawkins JD (1996) The social development model: a theory of antisocial behavior. In: Hawkins JD (ed) Delinquency and crime: current theories. Cambridge University Press, New York, pp 149–197
- Catalano RF, Haggerty KP, Hawkins JD, Elgin J (2011) Prevention of substance use and substance use disorders: the role of risk and protective factors. In: Kaminer Y, Winters KC (eds) Clinical manual of adolescent substance abuse treatment. American Psychiatric Publishing, Washington, DC, pp 25–63
- David-Ferdon C, Hammond WR (2008) Community mobilization to prevent youth violence and to create safer communities. Am J Prev Med 34:S1–S2
- Fagan AA, Hanson K, Hawkins JD, Arthur MW (2008) Implementing effective community-based prevention programs in the Community Youth Development Study. Youth Violence Juvenile Justice 6:256–278
- Fagan AA, Hanson K, Hawkins JD, Arthur MW (2009) Translational research in action: implementation of the Communities That Care prevention system in 12 communities. J Community Psychol 37:809–829
- Fagan AA, Arthur MW, Hanson K, Briney JS, Hawkins JD (2011a) Effects of Communities That Care on the adoption and implementation fidelity of evidence-based prevention programs in communities: results from a randomized controlled trial. Prev Sci 12:223–234
- Fagan AA, Hawkins JD, Catalano RF (2011b) Engaging communities to prevent underage drinking. Alcohol Res Health 34:167–174
- Feinberg ME, Bontempo DE, Greenberg MT (2008) Predictors and level of sustainability of community prevention coalitions. Am J Prev Med 34:495–501
- Gloppen KM, Arthur, MW, Hawkins, JD, Shapiro, VB (2012) Sustainability of the Communities That Care prevention system by coalitions participating in the Community Youth Development Study. J Adolesc Health 51:259–264
- Hallfors D, Cho H, Livert D, Kadushin C (2002) Fighting back against substance abuse: are community coalitions winning? Am J Prev Med 23:237–245
- Hawkins JD, Catalano RF Jr et al (1992a) Communities That Care: action for drug abuse prevention, 1st edn. Jossey-Bass, San Francisco
- Hawkins JD, Catalano RF, Miller JY (1992b) Risk and protective factors for alcohol and other drug problems in adolescence and early adulthood: implications for substance-abuse prevention. Psychol Bull 112:64–105
- Hawkins JD, Brown EC, Oesterle S, Arthur MW, Abbott RD, Catalano RF (2008a) Early effects of Communities That Care on targeted risks and initiation of delinquent behavior and substance use. J Adolesc Health 43:15–22
- Hawkins JD, Catalano RF, Arthur MW, Egan E, Brown EC, Abbott RD, Murray DM (2008b) Testing Communities That Care: the rationale, design and behavioral baseline equivalence of the Community Youth Development Study. Prev Sci 9:178–190
- Hawkins JD, Oesterle S, Brown EC, Arthur MW, Abbott RD, Fagan AA, Catalano RF (2009) Results of a type 2 translational research trial to prevent adolescent drug use and delinquency: a test of Communities That Care. Arch Pediatr Adolesc Med 163:789–798
- Hawkins JD, Shapiro VB, Fagan AA (2010) Disseminating effective community prevention practices: opportunities for social work education. Res Soc Work Pract 20:518–527
- Hawkins JD, Oesterle S, Brown EC, Monahan KC, Abbott RD, Arthur MW, Catalano RF (2012) Sustained decreases in risk exposure and youth problem behaviors after installation of the Communities That Care prevention system in a randomized trial. Arch Pediatr Adolesc Med 166:141–148
- Johnston LD, O’Malley, PM, Bachman, JG (2000) The Monitoring the Future national survey results on adolescent drug use: overview of key findings, 1999 (NIH Publication No. 00-4690). National Institute on Drug Abuse, Bethesda
- Kuklinski MR, Briney JS, Hawkins JD, Catalano RF (2012) Cost-benefit analysis of Communities That Care outcomes at eighth grade. Prev Sci 13:150–161
- Merzel C, D’Affliti J (2003) Reconsidering community based health promotion: promise, performance, and potential. Public Health Matters 93:557–574
- Oesterle S, Hawkins JD, Fagan AA, Abbott RD, Catalano RF (2010) Testing the universality of the effects of the Communities That Care prevention system for preventing adolescent drug use and delinquency. Prev Sci 11:411–424
- Patton GC, Coffey C, Sawyer SM, Viner RM, Haller DM, Bose K, Vos T, Ferguson J, Mathers CD (2009) Global patterns of mortality in young people: a systematic analysis of population health data. Lancet 374:881–892
- Quinby RK, Fagan AA, Hanson K, Brooke-Weiss B, Arthur MW, Hawkins JD (2008) Installing the Communities That Care prevention system: implementation progress and fidelity in a randomized controlled trial. J Community Psychol 36:313–332
- Rhew IC, Brown EC, Hawkins JD, Briney JS (2013) Sustained effects of Communities That Care on prevention service system transformation. Am J Publ Health 103:529–535
- Ringwalt C, Vincus AA, Hanley S, Ennett ST, Bowling JM, Rohrbach LA (2009) The prevalence of evidence-based drug use prevention curricula in U.S. middle schools in 2005. Prev Sci 10:33–40
See also:
Free research papers are not written to satisfy your specific instructions. You can use our professional writing services to buy a custom research paper on any topic and get your high quality paper at affordable price.
ORDER HIGH QUALITY CUSTOM PAPER

Always on-time

Plagiarism-Free

100% Confidentiality

{kind=link}