
This sample Road Traffic Injuries Research Paper is published for educational and informational purposes only. If you need help writing your assignment, please use our research paper writing service and buy a paper on any topic at affordable price. Also check our tips on how to write a research paper, see the lists of health research paper topics, and browse research paper examples.
Global Burden
Road traffic injuries are a growing public health problem, affecting millions of people worldwide each year. The World Report on Road Traffic Injuries (Peden et al., 2004) highlighted that globally nearly 1.2 million people die and between 20 million and 50 million people are injured or disabled as a result of road traffic injuries each year, with the majority of deaths occurring in the Western Pacific and Southeast Asia (see Figure 1). In2002, road traffic injuries were ranked as the fourth leading cause of death in adults aged 15–59 years worldwide, and as the third leading cause of death in males aged 15–44 years (Mathers et al., 2003).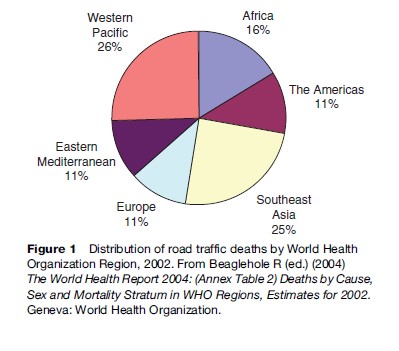
Demographic Groups At High Risk
Being male is a strong risk factor for many types of injury, including road traffic injury. Males account for 73% of all road traffic deaths worldwide (Peden et al., 2002), with an overall rate almost three times that for females (males: 27.6 per 100 000 population, females: 10.4 per 100 000 population). In low-income countries, there is a consistent predominance of male deaths over female deaths, with males comprising between 67% and 99.5% of road traffic deaths in these countries. About 70% of the disability-adjusted life years lost globally as a result of road traffic injury occurs among males. The gender differences are likely to reflect gender disparities in both exposure to road traffic injury risks and other risk-taking behaviors.
Age is also a strong risk factor for road traffic injury and death. High rates of fatalities are noted at both ends of the age spectrum, with increased rates for both younger drivers and older drivers. However, increased fatality rates in young drivers are due to a combination of factors including inexperience, distraction, and overconfidence, whereas the high fatality rates in older drivers are due to a range of factors including increased fragility.
High- Versus Low- And Middle-Income Countries
Although all regions in the world suffer from the epidemic of road traffic injuries, the low and middle-income countries bear a disproportionate burden of the injuries and fatalities (Ameratunga et al., 2006). According to World Health Organization data (Peden et al., 2004), these regions account for about 85% of traffic deaths each year. The overall road traffic injury fatality rate in2002 for low and middle-income countries was 20.2 deaths per 100 000 population, almost double the rate of 12.6 deaths per 100 000 population found in high-income countries.
Although in the last decades, the number of road traffic injuries has continued to rise in the world as a whole, time series analysis reveals the rates show clear differences in the pattern of growth between high-income countries and low-income and middle-income countries. There has been a steady decline in the fatality rates in high-income regions in the last three decades such as Australia, Canada, Germany, the Netherlands, Sweden, the United Kingdom, and the United States, while fatality rates are increasing in lowand middle-income regions as a result of rapid motorization and inadequate infrastructure to meet such increases. The magnitude of this increase varies by region, with the highest increase in Asia. Both the World Health Organization (Peden et al., 2004) and the World Bank (Kopits and Cropper, 2003) have predicted that in the next 20 years, without increased efforts, road traffic deaths will decline on average by almost 30% in high-income countries and increase by over 80% in low-income and middle-income countries. A 92% and 147% rise in fatalities is predicted in China and India, respectively.
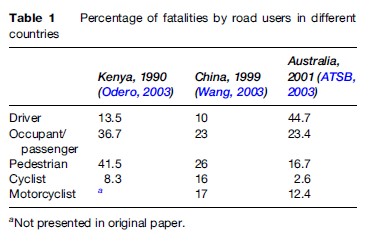
Road traffic crashes also disproportionately impact the poor and vulnerable members of society, particularly within low and middle-income countries. This is a reflection of the increased exposure of vulnerable groups to hazardous transport, for example as pedestrians, and as passengers traveling on the outside of vehicles such as buses and trucks. Such groups also have limited access to safety items such as seatbelts and helmets and advanced vehicle design features. Pedestrians, cyclists, motorized two and three-wheelers, and passengers in buses, minibuses, and trucks account for 90% of the casualties in low and middle-income countries because of the greater variety and intensity of traffic mix and the lack of separation from other road users, while in high-income countries drivers of automobiles constitute the majority of casualties (see Table 1). As motorization increases in countries such as China, fatalities will increasingly occur in drivers and passengers.
Children in low and middle-income countries are also disproportionately affected by road traffic injuries. Nantulya and Reich (2002) reported that among children aged 0–4 and 5–14 years, the number of road traffic fatalities per 100 000 population in low-income countries is approximately six times greater than in high-income countries.
Surveillance Systems
Measuring the burden of road traffic injuries is important so that governments may target solutions to groups at most risk. Well-constructed, validated, and reliable systems are evident in most high-income countries, using hospitalization data coded to International Classification of Disease (ICD) version 9 or 10. However, such systems are rare in low and middle-income countries. There are well-constructed guidelines for core data collections published by the World Health Organization.
It may not be possible to conduct surveillance reliably at all hospitals. As a result, some countries have developed systems whereby data are collected at selected hospitals (sentinel surveillance). In Thailand, for example, a surveillance system has been set up based on such a system. Although this system now operates as a national scheme, it originated as a provincial injury surveillance system based in five sentinel hospitals (Peden et al., 2004: 54). There are, however, few such systems in place in low or middle-income countries worldwide.
There are other methods for collecting the necessary data when national or regional health data collection systems are not in place. Use of injury reports from police-reported crash data may be used for surveillance, although such data are generally regarded as less reliable than hospital data, which are constructed from medical records by skilled coders. Other methods of surveillance include representative household surveys, used for example in Vietnam (Le et al., 2003) and Pakistan (Ghaffar et al., 2004), to document the burden of injury using stratified random household surveys. In both instances, these studies have highlighted the tremendous burden of injury caused by road traffic injury. Topic-specific surveys may also be carried out to establish prevalence of behaviors, for example, motorcycle helmet use surveys, where helmet use is recorded for all riders in a particular area.
Costs
Road crashes have a significant impact on the world economy, with global costs of road crashes estimated to be about $518 billion each year (Peden et al., 2004). The average annual cost of road crashes has been estimated to be about 1% of gross national product in developing countries, 1.5% in countries undergoing economic transition, and 2% in highly motorized countries ( Jacobs et al., 2000). Much of the cost of road traffic injury is due to nonfatal events, with the effects on lost productivity of nonfatal injury thought to outweigh that resulting from fatal injury. The true costs to society are likely to be far greater once indirect costs are factored in.
Although estimates of road-traffic-related injury and subsequent disability in low and middle-income countries are scarce, it is widely recognized that the consequences of road traffic crashes are a significant issue for such countries, pushing individuals deep into poverty. Zhou and colleagues (2003) estimated that in China, injury is the major source of potentially productive years of life lost, more than any other disease group. Productivity losses from injury, estimated to have an annual economic cost equivalent to US$12.5 billion, were found to outweigh the total productivity of new entrants to the labor market. Road traffic injuries accounted for 25% of all injury-related productivity losses, with an excessive loss of productivity in rural areas, resulting in a significant and negative impact on economic growth.
Intervention Strategies
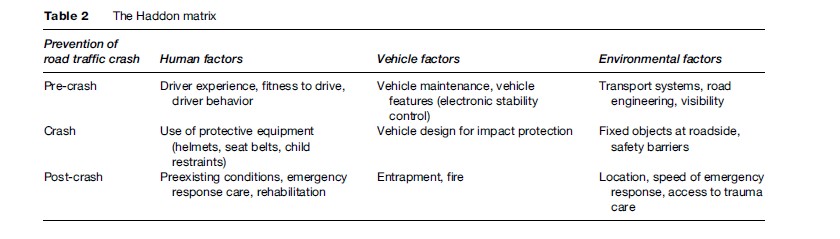
Successful programs aimed at reducing road traffic injury are based on the premise that road traffic crashes are predictable and therefore preventable. Both crash and injury rates have significantly declined in the past 20 years in high-income countries due to a combination of strategies ensuring safer drivers, safer roads and transport systems, and safer vehicles. This was aided by the development of the Haddon matrix (see Table 2), a conceptual model in which the principles of public health were applied to the problem of traffic safety. This approach led to substantial advances in the understanding of the behavioral, road-related, and vehicle-related factors that affect both the number and severity of road traffic-related injuries.
Following on from this, many agencies worldwide, including both the World Health Organization and the World Bank, advocate a systems approach to road safety. This approach addresses the traffic system as a whole and examines the interactions between road users, the road infrastructure and transport systems, and vehicles to identify effective solutions.
Road Users
In high-income countries, legislated interventions that relate to improving safety in drivers such as blood alcohol limits for drivers, licensing and registration systems, lower speeding limits, and mandatory restraint and helmet laws have been tremendously successful in reducing the numbers of crashes and hence injuries on the roads. For legislated interventions to be successful, it is widely recognized that they need to be vigorously enforced and accompanied by community-wide social marketing and education campaigns.
Blood Alcohol Limits
It has been recognized for many years that drivers who have consumed alcohol have a far higher crash risk than those who have not. The relative risk of a crash increases with increasing blood alcohol level for drivers of cars, and alcohol also increases the risk of fatal crashes for both riders of two-wheelers and pedestrians. As a result, many high-income countries have limited legal blood alcohol limits for experienced drivers to 0.05mmol/l, with zero blood alcohol allowed for drivers of commercial passenger vehicles. Decreases in mandated driver blood alcohol limits have been shown to be effective in terms of reducing death and injuries in a numbers of settings worldwide (Shults et al., 2001).
Young drivers have an even higher risk of crash and injury associated with high blood alcohol concentration than more experienced drivers. Recognition of this increased risk is reflected in the zero blood alcohol restrictions for young drivers in some graduated licensing schemes. Such restrictions are supported by research such as that published by Shults et al. (2001), demonstrating reductions in crashes of between 4% and 24% with low mandated blood alcohol limits for young drivers.
Blood alcohol legislation is generally enforced using sobriety checkpoints, or road-side random breath testing, accompanied by widespread social marketing and education. Random breath testing has been shown to be one of the most cost-effective safety interventions known, with a cost–benefit ratio of 1:19 (Peden et al., 2004).
Licensing And Registration Systems
Implementation of mandatory licensing and registration systems for drivers and cars is also essential to road safety. In addition to providing a structure such that numbers of drivers and vehicles, driver training, and vehicle maintenance can be monitored, such systems also provide a mechanism for issuance of infringement notices and penalties. Importantly, the revenue accrued can be channeled back into appropriate infrastructure and road safety.
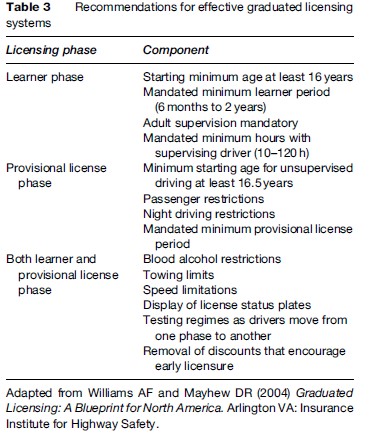
Graduated licensing for novice drivers has also been successful in reducing road traffic injuries in younger age groups in high-income countries (Williams and Mayhew, 2004). This licensing structure implemented in many states in the United States, Canada, Australia, and in New Zealand aims to reduce exposure of inexperienced drivers to high-risk driving situations. Limitations of the systems vary by jurisdiction, but may include extended learner periods, minimum supervised driving hours during the learner period (ranging from 10 to 120 hours) zero blood alcohol requirements, limited maximum speed, and passenger and night driving restrictions (Table 3). Such systems have been shown to be very effective in reducing the overrepresentation of young drivers in road traffic crashes.
Speed Control
Speed has been identified as one of the key risk factors contributing to road traffic injuries. Speed affects both the risk of being involved in a crash and the severity of the injuries caused. At higher speeds, the driver has less time to respond to a sudden event, the stopping distance is increased, and the likelihood of crashing is therefore increased. Injury severity in a crash rises sharply with the speed of the vehicle in a collision, reflecting the laws of physics.
Speeding is very common among drivers, with almost all motorists, at some stage during their driving career, exceeding the recommended or posted speed limit. In some high-income countries such as the United States and Australia, it is estimated that speed contributes to about 30% of deaths on the road. The situation is similar in low and middle-income countries; for example Afukaar (2003) reported that speed was identified as the main contributory factor in 50% of road crashes in Ghana between 1998 and 2000.
There is a large amount of empirical evidence on the impact of speed on both the likelihood of crashing and the severity of injury. For example, Finch et al. (1994) highlights that an average increase in speed of 1 km/h is associated with a 3% higher risk of a crash involving an injury, and a 4–5% increase in fatal crashes, and Kloeden et al.’s study of crashes (1997) within 60 km/h speed limit zones showed the risk of involvement in a casualty crash doubles with each 5-km/h increase in traveling speed above 60 km/h. As well, increases in mandated speed limits increase the risk of crashes and subsequent injuries. Following the raise in speed limits in 1987 on U.S. rural interstates from 55 to 65 mph, there was a 2to 3-mph (or 4.8%) increase in mean traffic speeds and a 21% increase in fatalities. In 1995, following the second round of raised speed limits, average interstate speeds and deaths increased in many U.S. states by 4% and 17%, respectively, indicating that small increases in the speed limit resulted in a dramatic increase in road fatalities.
Speed of traffic is also an issue for pedestrians and other vulnerable road users. Pedestrians have a high chance of surviving a car crash at low speeds but the fatality rate rapidly increases to 100% with increased speed of vehicle on impact. Reflecting the vulnerability of pedestrians and other vulnerable road users, many countries worldwide now have a general urban speed limit of 50 km/h.
It is generally recognized that setting appropriate speed limits and enforcing them is important in reducing speed-related road traffic injuries. Jurisdictional authorities worldwide use various criteria in determining appropriate speeds for roads to ensure consistent and credible speeds. These may include such factors as the width and quality of the road, traffic and pedestrian volume, the environment in which the road is located, presence of traffic signals and pedestrian crossings, and type of roadside activities.
There are a number of ways that speed can be managed. Interventions such as speed enforcement detection devices (for example, fixed or mobile speed cameras), widely implemented in some high-income countries such as the UK to enforce speed limits and keep average speeds down, have been shown to be effective tools in the prevention of crashes and injuries (Pilkington and Kinra, 2005). Traffic calming (the use of physical structures on roads used to reduce vehicle speeds) is another strategy used to limit speed of traffic, particularly cost-effective in both high and low-income countries if implemented at the time when roads are first constructed. In-vehicle speed limiting devices are also used worldwide to manage speed in heavy vehicles and public transport vehicles.
With the current trend in the production of modern vehicles with high-speed capacity, effective management of speed will remain an important issue in both high and low-income countries.

Driver Education And Training
There are several types of driver education and training, including school-based road safety education, pre and post-license driver training courses taught by professional instructors, and one-to-one driving instruction with professional instructors that is provided during the learner phase. There has been substantial research evaluating the benefits of such programs, some of this summarized in systematic reviews. One review found that school-based driver education resulted in increased exposure with no advantage in terms of crash reduction (Roberts et al., 2001); another found no safety benefits for post-license driver education (Ker et al., 2003). There is also evidence that courses that teach advanced driving skills such as skid handling to novice drivers may in fact increase crash rates, possibly due to the development of a false confidence in the driver’s ability.
Overall, there is little research evidence that pre or post-license driver education or training has a positive effect on driver behavior or on crash and injury rates. However, driving instruction during the learner phase by professional driving instructors is thought to make a useful contribution to the development of driving skills. Given the widespread participation in driver education and training courses worldwide, continued research on efficacy of such courses is necessary.
Road Safety Education
In most high-income countries, road safety is taught at schools as part of normal curricula from the first year of school. A number of evaluations of school-based education programs aimed at primary school children have shown that it is possible to improve the pedestrian skills of children and to modify the abilities of parents to assess accurately the skills of their children in crossing streets. The key features of these programs are that they include cross-curricula education, activities that increase practical road crossing skills and importantly, they advocate that children are assisted by an adult when crossing a road until the age of 10 years. Educational programs to improve road user behaviors in teenagers, however, have shown less success. There have been no comprehensive well-controlled evaluations of school-based road safety education programs aimed at high-school-aged children that have demonstrated improvements in road user behaviors. As with driver training, there is a need for well-controlled evaluations of implemented programs.
Seat Belt And Motorcycle Helmet Legislation
Ensuring compliance with legislation such as seat belt and motorcycle helmet legislations is also a vital aspect of road safety (Figure 2). There is abundant evidence as to the effectiveness of both seat belts (Marine et al., 1994) and motorcycle helmets (Liu et al., 2004) in terms of preventing death and injury in the event of a crash. Most high-income countries worldwide have national seat belt and helmet legislation, which is generally enforced and complied with. In countries such as Australia and New Zealand, seat belt use is close to 95% but despite this up to 30% of serious injury crashes involve an unrestrained person. A notable exception to consistent national legislation is the United States, where a combination of political and historical events has resulted in variable legislation across the states, with resulting variations in seat belt and helmet-wearing rates. However, in general, seat belt-wearing rates are as high as 90–99% for front seat occupants in high-income countries, whereas in low and middle-income countries the rates are much lower. The pattern is similar for motorcycle helmets, with wearing rates around 90% in countries where helmet legislation is enforced, but less than 20% where it is not. There is a vibrant road-side market for motorcycle helmets in many low-income countries, but many of these helmets have no impact-absorbing materials (for example, a foam inner liner) and may confer no benefits to the user in the event of a crash.
There are many challenges to improving seat belt and helmet-wearing rates in low and middle-income countries. Some of these include ensuring that cars are fitted with both front and rear seat belts and that high-quality but affordable helmets are available.
Driver distraction
Factors that cause driver distraction include use of mobile phones, as well as passengers, music, and use of other technology such as satellite navigation systems. Passenger restrictions for novice drivers reflect the increased crash risk that peer passengers pose for this at-risk driving group. With respect to mobile phones, laboratory studies have shown than driving performance is affected by both hand-held and hands-free mobile phones (McCartt et al., 2006). Recent population studies have confirmed that use of hands-free phones confer similar risk of involvement in injurious crashes as hand-held phones – with roughly a fourfold increase irrespective of age. While the specific impact on crashes of in-car communication and navigation devices including voice activation software is presently unclear, laboratory studies indicate that the cognitive load on the driver using such devices has a significant impact on driving performance.
There is a clear need for further research on the effect of driver distraction on crash risk. Although results are not yet available, there are currently a number of naturalistic driving studies underway worldwide; such studies record in-car activity and are able to assess the contribution of various distracting factors to crash risk. These studies will add to the body of research on driver distraction and aid the development of effective countermeasures.
Research on driver distraction has largely been confined to high-income countries, although the increased crash risk due to driver distraction is likely to be similar in other settings. However, there has been little research in any setting examining use of mobile phones on two-wheelers and mopeds, and given the widespread and increasing use of mobile phones and portable music devices, it seems likely that driver distraction will be a major safety issue in low and middle-countries in the future where such forms of transport are very common.
Fatigue Management
Estimates of the proportion of road traffic injuries that are attributed to fatigue or sleepiness vary, but range from a few percent to more than one-third of all crashes, depending on the definition used. Research from New Zealand has shown that acute sleepiness in drivers is associated with a significant increased risk of serious injury crashes (Connor et al., 2002). Fatigue is recognized as a particular issue in the road freight industry, a work environment for which there are many challenges, including vast distances, tight delivery schedules, low, unregulated freight rates, and penalties for late delivery. Consequently, extended driving schedules and the need to meet deadlines may contribute to a variety of factors affecting driving behavior; including fatigue, stress, and the use of stimulants in order to stay awake.
Interventions used to manage fatigue include social marketing and community education, as well as use of legislation mandating the maximum number of permitted driving hours for commercial drivers. Enforcement of such laws relies on use of log books and in some cases technology such as cameras to track heavy-vehicle drivers. In some countries, including Australia, stringent chain of responsibility legislation has also been passed ensuring that all parties in the road transport supply chain have specific obligations under the law to prevent a breach of transport law including driving hours.
Road And Transport Systems
Building road safety into road engineering, urban design, and transport planning is vital for reductions in road traffic injury. With rapid motorization and increased road building in low and middle-income countries, this will become more of an issue in the decades to come.
Improved road engineering has contributed significantly to reduced crash and fatality rates in high-income countries in the past two decades, partly because such improvements work without dependence on behavioral change of individuals. Building high-quality, appropriately signposted roads is a major priority for governments around the world. Implementation of improved engineering solutions such as safer roadside barriers such as guardrails and crash cushions have been shown to be very effective in reducing both the number and severity of crashes; however, building and upgrading roads is an enormous cost for both high and low-income countries.
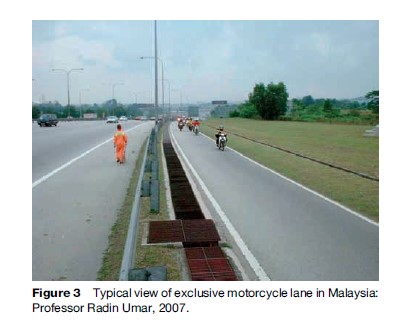
Road building in countries undergoing rapid motorization also needs to take account of the needs of vulnerable road users. It is vital that road safety measures are taken into account: examining traffic mix and developing transport systems so that fast-moving traffic is separated from slow-moving traffic and vulnerable road users. Where traffic contains a diverse mix of vehicles moving at very different speeds, there is clearly more potential for crash and injury. Vulnerable road users are most at risk and systems in various jurisdictions have been developed in order to separate out the traffic flow with some success, such as dedicated motorcycle lanes in Malaysia (Figure 3). However, careful planning is essential as badly lit or minimally frequented tunnels and overpasses for motorcyclists and pedestrians may also provide opportunities for bandits and robbers. Similarly, findings from countries such as Brazil, Mexico, and Uganda suggest that where pedestrian overpasses have a high perceived risk of personal crime, pedestrians will not use them, choosing instead to walk through the traffic, resulting in an increased risk of road traffic injury (Ameratunga et al., 2006).
Consideration of road safety in urban planning and development of transport policy is also important. For example, as outlined in the World Health Report (Peden et al., 2004) investment in safer transport systems is a crucial component of road safety systems. Mass transit public transport systems have far lower fatality and injury rates than personal transport systems, and also bring other benefits, such as the obvious environmental benefits of minimizing numbers of private vehicles.
Transport planning includes managing exposure to risk, as reduction in distance traveled is associated with reductions in crashes. This may mean encouraging people to use low-risk forms of transport, priority to higher occupancy vehicles such as buses, placing limitations on motor vehicle use, as well as land planning, which among other things ensures that transport corridors are short and well placed and that there are alternatives to private transport.
Finally, incorporating safety into road planning is crucial. Having good road design, appropriate speed limits for the road type and roads engineered for safety contributes to low crash and injury rates. For example, high-speed roads, such as expressways have physical separation of traffic in opposing directions, high-quality surfaces and clear space on the road side. Having lower speeds set for local roads and area-wide traffic calming systems such as rumble strips and speed bumps, traffic redistribution, and changes to the road environment all contribute to a lower incidence of crash and serious injury (Bunn et al., 2003). Additionally, having crash-protective road sides whereby trees, light poles, and other roadside furniture are minimized further reduces the likelihood of crash and injury.
Vehicles
Improvements in vehicle design over the past few decades have been credited with saving thousands of lives (Peden et al., 2004). Use of cars with advanced safety features can both prevent crashes from occurring and result in fewer injuries and deaths once crashes have occurred. For example, use of electronic stability control results in a reduction in crashes and interventions such as seat belts and airbags prevent serious injuries.
Improvements in other car design features have also had an impact on crash reduction, such as designing the car front so as to minimize injury to vulnerable road users such as pedestrians in the event of a crash. Such car designs may include space under the hood giving sufficient clearance between the hood and the engine components below to minimize head impacts; laminated windscreens; smoother, recessed, and softer bumpers; and external airbags to minimize other injuries. Modifications to truck design such as energy-absorbing front, rear, and side under-run protection also decrease deaths by preventing under-running of cars under trucks.
Devices to improve visibility such as lights and bright materials increase visibility of pedestrians and cyclists (Kwan and Mapstone, 2006) and may result in decreased injuries. High mounted brake lights in cars reduce rear end crashes by between 15% and 50% and are generally now incorporated as part of the base model in new vehicles, at least in high-income countries (Peden et al., 2004).
Use of child restraints is also mainly confined to high-income countries where the majority of travel occurs in private cars. Such restraints are very effective in reducing injury to children in the event of a crash, but most available for infants are dependent on the presence of working seat belts and bolts. There is a clear need for work in improving use of child seats in vehicles in low and middle-income countries, particularly in countries such as Vietnam where children often ride on motorcycles as passengers or as babies in arms.
Even in high-income countries, advanced safety features in cars are not always sold as part of the base model, with manufacturers allowing consumers to opt in for such packages. In low-income countries, cars are often sold without even seat belts, and in some cases imported cars are decommissioned for the market with seat belts and other safety devices removed before point of sale. As motor vehicles are on the road for many years after they are sold, it is important that car manufacturers ensure that safety features are included as part of the base model rather than as add-ons.
Many developing countries manufacture locally de- signed vehicles for example, tuk-tuks (Thailand, Laos, Cambodia), becaks (Indonesia), and jeepneys (Philippines). These vehicles generally are used as taxis but are designed with few concerns for crash performance or road safety. It may not be possible or reasonable to impose international safety standards on them due to the local social and economic contexts; however, steps should be taken to make them safer for drivers and other road users.
Translation Of Research From High-Income To Low And Middle-Income Settings
The reductions in road traffic fatalities in high-income countries are attributed largely to the implementation of a wide range of road safety measures, including seat belt use, vehicle crash protection, traffic calming interventions and traffic law enforcement. Many of these strategies are slowly being implemented into low and middle-income countries, but there is much work to be done to ensure that this process occurs in a timely and appropriate manner (Ameratunga et al., 2006).
There are many differences between countries worldwide that influence whether known effective interventions may be replicated or effectively transferred to other settings. These include differences in traffic mix and cultural, socioeconomic, and political settings. These may create substantial difficulties, both philosophically and administratively, in implementing interventions in low-income countries. Issuing fines requires an administrative system to administer and collect the fine, and individuals may not have postal addresses at which they receive mail. Corruption of officials may mean fines are circumvented by bribery. Furthermore, having police and administrative staff available to administer the laws may be a drain on limited resources, particularly where policing is overwhelmed with violent crime and other more acute issues. There is therefore a need for policy makers at the country level to recognize that the prevention of road traffic injuries is a high priority and design and evaluate effective intervention strategies and policies based on local circumstances.
Furthermore, what may have been proven to be effective in a high-income setting may not necessarily be effective in a low-income setting. This means that when introduced to a low-income setting, policy and interventions used in high-income settings must be carefully evaluated and adapted where appropriate.
The Future
Although there have been dramatic improvements in road safety in high-income countries worldwide, for most of the world’s population the burden of road traffic injury is growing rapidly. For those in high-income countries, reductions in road injury will continue to be made with safer drivers, better road engineering and transport systems, and increased vehicle safety. Increases in both in-car and out-of-car technology will aid this. However, there will also be a continuing need for governments to manage road users and ensure development and compliance with appropriate legislation.
There is however, an urgent need for both surveillance and high-quality controlled intervention research examining ways in which proven road safety interventions and technology can be implemented in low-income country settings. While there are well-developed systems for training of specialists in the area in high-income countries, there is a great need for capacity building in terms of human resources in low and middle-income countries. Training and continued support, both financial and intellectual, are vital for developing a vital in-country workforce, including policy makers, jurisdictional authorities, police, and researchers.
Many countries have recognized the need for multispectral collaboration on road safety. Raising awareness of the consequences of road traffic injury, incorporation of road safety into national planning, and collaboration between key stakeholders in transport, health, and industry worldwide is vital in ensuring that road traffic injuries are managed appropriately. A global, multispectral, and multidisciplinary approach as advocated by the World Health Organization (Peden et al., 2004) is urgently needed to ensure that the epidemic of road traffic injuries worldwide is slowed.
Bibliography:
- Afukaar FK (2003) Speed control in developing countries: issues, challenges and opportunities in reducing road traffic injuries. Injury Control and Safety Promotion 10(1–2): 77–81.
- Ameratunga S, Hijar M, and Norton R (2006) Road-traffic injuries: Confronting disparities to address a global-health problem. Lancet 367: 1533–1540.
- Australian Transport Safety Bureau (2003) Road Fatalities Australia: 2002 Statistical Summary. Canberra, Australia: Australian Transport Safety Bureau.
- Beaglehole R (ed.) (2004) The World Health Report 2004: (Annex Table 2) Deaths by Cause, Sex and Mortality Stratum in WHO Regions, Estimates for 2002. Geneva, Switzerland: World Health Organization.
- Bunn F, Collier T, Frost C, et al. (2003) Area-wide traffic calming for preventing traffic related injuries. Cochrane Database of Systematic Reviews, Issue 1.: CD003110.
- Connor J, Norton R, Ameratunga S, et al. (2002) Driver sleepiness and risk of serious injury to car occupants: Population based case control study. British Medical Journal 324: 1125.
- Finch DJ, Kompfner P, Lockwood CR, and Maycock G (1994) Speed, Speed Limits and Accidents. Crowthorne, UK: Transport Research Laboratory.
- Ghaffar A, Hyder AA, and Masud TI (2004) The burden of road traffic injuries in developing countries: The 1st national injury survey of Pakistan. Public Health 118(3): 211.
- Jacobs G, Aeron-Thomas A, and Astrop A (2000) Estimating global road fatalities (Report 445). Crowthorne, UK: Transport Research Laboratory.
- Ker K, Roberts I, Collier T, et al. (2003) Post-licence driver education for the prevention of road traffic crashes. Cochrane Database of Systematic Reviews Issue 3.: CD003734.
- Kloeden CN, McLean AJ, Moore VM, and Ponte G (1997) Travelling Speed and the Risk of Crash Involvement. Adelaide, Australia: NHMRC Road Accident Research Unit, The University of Adelaide.
- Kopits E and Cropper M (2003) Traffic Fatalities and Economic Growth. The World Bank: Development Research Group Infrastructure and Environment, Policy research working paper 3035. Washington DC: The World Bank.
- Kwan I and Mapstone J (2006) Interventions for increasing pedestrian and cyclist visibility for the prevention of death and injuries. Cochrane Database of Systematic Reviews, Issue 4.: CD003438.
- Le AV, Le LC, and Pham CV (2003) Vietnam Multi Center Injury Survey: Primary Results. Hanoi, Vietnam: Hanoi School of Public Health.
- Liu B, Ivers R, Norton R, Blows S, and Lo SK (2004) Helmets for preventing injury in motorcycle riders. Cochrane Database of Systematic Reviews Issue 2.: CD004333.
- Marine WM, Kerwin EM, Moore EE, et al. (1994) Mandatory seatbelts: Epidemiologic, financial, and medical rationale from the Colorado matched pairs study. Journal of Trauma 36(1): 96–100.
- Mathers CD, Bernard C, Moesgaard Iburg K, et al. (2003) Global Burden of Disease in 2002: Data Sources, Methods and Results. Global Programme on Evidence for Health Policy Discussion Paper No. 54. Geneva, Switzerland: World Health Organization.
- McCartt AT, Hellinga LA, and Bratiman KA (2006) Cell phones and driving: Review of research. Traffic Injury Prevention 7(2): 89–106.
- Nantulya VM and Reich MR (2002) The neglected epidemic: Road traffic injuries in developing countries. British Medical Journal 324: 1139–1141.
- Odero W, Khayesi M, and Heda PM (2003) Road traffic injuries in Kenya: Magnitude, causes and status of intervention. Injury Control and Safety Promotion 10(1–2): 53–61.
- Peden M, McGee K, and Sharma G (2002) The Injury Chart Book: A Graphical Overview of the Global Burden of Injuries. Geneva, Switzerland: World Health Organization.
- Peden M, Scurfield R, and Sleet D (2004) World Report on Road Traffic Injury Prevention. Geneva, Switzerland: World Health Organization.
- Pilkington P and Kinra S (2005) Effectiveness of speed cameras in preventing road traffic collisions and related casualties: Systematic review. British Medical Journal 330(7487): 331–334.
- Roberts I and Kwan I; Cochrane Injuries Group Driver Education Reviewers (2001) School-based driver education for the prevention of traffic crashes. Cochrane Database of Systematic Reviews, Issue 3.: CD003201.
- Shults RA, Elder RW, Sleet DA, et al. (2001) Reviews of evidence regarding interventions to reduce alcohol-impaired driving. American Journal of Preventive Medicine 21(4S): 66–88.
- Wang SY, Chi GB, Jing CX, et al. (2003) Trends in road traffic crashes and associated injury and fatality in the People’s Republic of China, 1951–1999. Injury Control and Safety Promotion 10(1–2): 83–87.
- Williams AF and Mayhew DR (2004) Graduated Licensing: A Blueprint for North America. Arlington, VA: Insurance Institute for Highway Safety.
- Zhou Y, Baker TD, Rao K, and Li G (2003) Productivity losses from injury in China. Injury Prevention 9(2): 124–127.
- Farmer CM and Lund AK (2006) Trends over time in the risk of driver death: What if vehicle designs had not improved? Traffic Injury Prevention 7(4): 335–342.
- Hartling L, Wiebe N, Russell K, et al. (2004) Graduated driver licensing for reducing motor vehicle crashes among young drivers. Cochrane Database of Systematic Reviews Issue 2.: CD003300.
- Mohan D (2002) Road safety in less motorized environments: Future concerns. International Journal of Epidemiology 31: 527–532.
See also:
Free research papers are not written to satisfy your specific instructions. You can use our professional writing services to buy a custom research paper on any topic and get your high quality paper at affordable price.
ORDER HIGH QUALITY CUSTOM PAPER

Always on-time

Plagiarism-Free

100% Confidentiality



