
This sample Treatment of Sex Offenders Research Paper is published for educational and informational purposes only. If you need help writing your assignment, please use our research paper writing service and buy a paper on any topic at affordable price. Also check our tips on how to write a research paper, see the lists of criminal justice research paper topics, and browse research paper examples.
This research paper gives a brief overview on the effects of sexual offender treatment drawing on evidence from a number of meta-analyses and systematic reviews. Overall, this research reveals a positive effect on sexual reoffending. The syntheses suggest a mean effect of approximately d = 0.20 ± 0.10. Because of the low base rate of sexual reoffending, this equals about 25 % less recidivism of treated offenders as compared to untreated groups. However, the studies and findings are extremely heterogeneous and outcomes vary depending on many program, setting, offender, and methodological factors.
Unfortunately, the quality of the majority of evaluation studies on sex offender treatment is rather weak. However, the overall design quality is not consistently related to effect sizes, and the same applies to various other methodological and content characteristics. Cognitive-behavioral treatment, relapse prevention, and programs that adhere to the Risk-Need-Responsivity Model show relatively consistent positive effects, although even such interventions sometimes fail to demonstrate positive effects. Hormonal medication for subgroups of sexual offenders is promising, too, but it needs more methodologically sound evaluations on this topic. By trend, programs in ambulatory settings, with some individualization and proper implementation, and for offenders at higher risk of reoffending, show above-average effects.
The small number of methodologically sound studies with specific characteristics and confounded moderator variables makes it difficult to draw robust conclusions. Despite practical problems in undertaking randomized experiments in this area, more high-quality evaluations are highly needed.
Introduction
In many countries sexual offending is a topic of particularly high concern in the general public and the media. Accordingly, governments implemented two main strategies to deal with sex offenders. On the one hand, they put into effect tougher sentences and security measures for this offender population. On the other hand, they invested in sexual offender treatment programs to reduce reoffending. Although treatment of sexual offenders became common in many Western countries, there is much controversy about its effectiveness (Marshall & Marshall 2010; Rice & Harris 2003). A consensus on “what works” in sexual offender treatment is complicated by various issues. First, sexual offending is a very heterogeneous category that contains, for example, various forms of child molesting, rape, exhibitionism, distribution, and consumption of child pornography in the internet. Second, there are very different types of sexual offenders such as those with or without a deviant sexual preference (paraphilia), an antisocial personality, an opportunistic orientation, and neuropsychological deficits. Third, although much research on risk factors for reoffending and structured assessment instruments has been carried out, the evidence on the causal mechanisms is less clear. Fourth, treatment approaches are very heterogeneous ranging from cognitive-behavioral programs and relapse prevention over psychodynamic approaches and multi-systemic therapy to hormonal treatment by medication or surgical castration, and some of these categories embrace rather different approaches in themselves (McGrath et al. 2010). Fifth, sound treatment evaluation of routine practice is difficult because in many jurisdictions serious sexual offenders cannot simply be left untreated in control groups and sexual reoffending requires rather long follow-up periods.
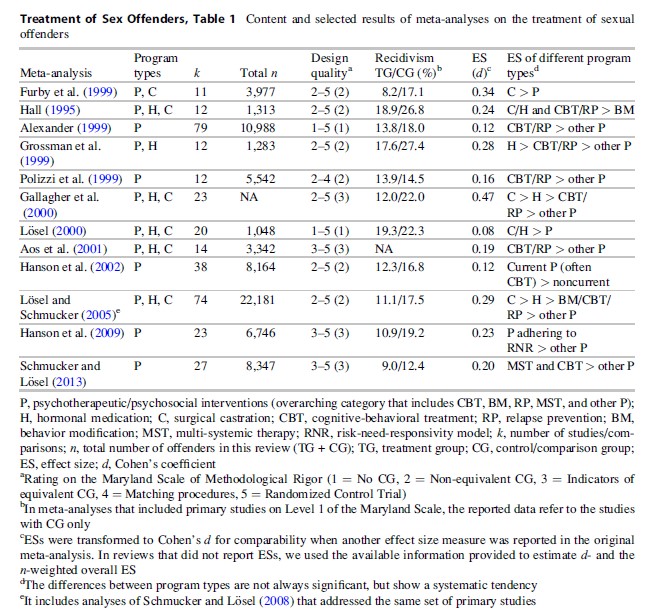
Accordingly, compared to general or violent offender treatment, methodologically sound evaluations of programs for sexual offenders are less frequent, particularly outside North America (Lipsey and Cullen 2007; Losel 2012). However, since the 1990s, controlled evaluations have increased and a number of systematic reviews and meta-analyses could be carried out. Table 1 summarizes important features and findings of 12 reviews and meta-analyses that (a) mainly addressed adult sexual offenders, (b) used sexual reoffending as outcome measure (e.g., arrest, conviction, incarceration, or self-reported offenses), and (c) calculated effect sizes (ES) or at least provided systematic data that can be used for effect size estimations. Concentrating on meta-analyses reduces problems of selective file drawing and subjective evaluation. A focus on effect size instead of mere statistical significance provides more adequate information because many sex offender treatment studies contain rather small samples and thus lack statistical power. The remaining entry will provide a brief overview of the main findings and the controversies that arise from those research integrations. Although there is overlap between these syntheses, they vary substantially with regard to the included primary studies, categories for coding, methods of data analysis, calculation and integration of effect sizes, and investigation of outcome moderators.
Some meta-analyses concentrated on psychotherapeutic/psychosocial interventions only. Others also included hormonal treatment by medroxyprogesterone-acetate or cyproteroneacetate to reduce male sexual hormones as well as surgical castration. In the general category of psychotherapeutic/psychosocial interventions, the individual treatment programs vary considerably and contain interventions such as behavior modification, cognitive-behavioral treatment (CBT), relapse prevention, psychodynamic approaches, social therapy, or multi-systemic therapy. Some of these intervention types share similarities. For example, the contents of CBT (e.g., reducing deviant sexual attitudes, improving self-control, enhancing social skills, promoting perspective taking, or coping with stressors) overlap with those of relapse-prevention programs that focus more strongly on risk situations and fantasies of offenders with a deviant sexual orientation (paraphilia). And multi-systemic therapy for young sexual offenders and social therapy/therapeutic communities make particular use of the social context of the clients but also incorporate elements from CBT or psychodynamic approaches. Hormonal treatment is primarily used for those offender subgroups who are mainly motivated by sexual drive (and not by dominance, etc.), but the medication is often accompanied by CBT or other psychosocial interventions.
Table 1 also presents the methodological quality of the included primary studies using a slightly modified version of the Maryland Scale of Methodological Rigor (MSMR; Farrington et al. 2002) which has five levels: Level 1: Only treatment group (TG) data, no control or comparison group (CG); Level 2: Nonequivalence of TG and CG, differences on relevant variables effecting recidivism are reported or are to be expected (e.g., treatment dropouts or nonstarters); Level 3: Incidental assignment but equivalent CG, sound statistical control, or empirical data on equivalence in relevant variables; Level 4: Matching procedures, systematic strategy to attain equivalence of TG and CG; and Level 5: Random assignment of subjects to TG and CG, no selective dropout.
Most meta-analyses contain a majority of studies that are rather weak methodologically (Levels 1 and 2). This is a serious problem because the results from such studies can be distorted. However, while high internal validity is a precondition for any causal inference and generalization, an exclusive reliance on randomized controlled trials (RCTs) would lead to a very narrow database. For example, a Cochrane review of RCTs on sex offender treatment ended up with only three studies on very different modes of treatment (White et al. 2009). Thus, hardly any conclusion could be drawn except stating the lack of RCTs. A review of Brooks-Gordon et al. (2006) contained nine RCTs, but the majority did not use reoffending as outcome measures. Most recently Schmucker and Losel (2013) found six RCTs on sexual offender treatment with offending as outcome. However, the findings of these studies were very different and did not reveal a clear picture that could guide practice and policy making. It is necessary to conduct more RCTs in the evaluation of sexual offender treatment. But one has to be aware of the practical problems in implementing and maintaining an RCT in this research area. One should also take into account that methodological quality is a multidimensional category and sound quasi-experiments can provide useful information (Losel 2007). Against this background it seems helpful not yet to ignore findings from suboptimal studies on sexual offender treatment.
In total, the meta-analyses indicate a substantial increase of evaluations in the 1990s and 2000s. The large number of studies and high n in Alexander (1999) is due to the inclusion of methodologically weak studies without comparison groups. The increase in evaluation research is also accompanied by better design quality. As the most recent review of Schmucker and Losel (2013) shows, nearly half of the studies at Level 3 or above of the MSMR have been published in the 2000s. Perhaps, the public concern about sexual offending led to more interest in sound evidence and research funding in this field. However, one must bear in mind that even the recent evaluation reports do not necessarily address the most recent programs. Sexual reoffending has a relatively low base rate and often only occurs after rather long time periods. Therefore, many evaluations of sexual offender treatment have rather long follow-up periods. Whereas in the evaluation of general offender treatment a follow-up of 1–2 years is frequent, the average follow-up in most meta-analyses reported in Table 1 is clearly over 4 years, ranging to more than 20 years for individual primary studies. This is a positive feature of the respective primary research, but it also has the implication that completed evaluations often address programs that have been revised in the meantime.
In all meta-analyses, except for Losel (2000) which integrated German studies, the majority of included evaluations came from North America. This may be partially a consequence of the focus on English-language reports by native English-speaking authors. However, similar to other fields of correctional treatment, the dominance of the United States and Canada also reflects a stronger evidence orientation and research activity in the Anglo-American World. It is good news that some meta-analyses on sexual offender treatment also found sound evaluation research in other parts of the world. For example, in the most recent review, approximately one third of the eligible studies stem from outside North America. Despite this positive tendency there are still too few studies from different countries to draw conclusions about the impact of the cultural or legal framing conditions on the effects of sexual offender treatment.
Overall Effect
All meta-analyses suggest a desirable mean effect of sexual offender treatment. The average rates of sexual recidivism in treated offenders varied between 8.2 % (Furby et al. 1989) and 19.3 % (Losel 2000). In contrast, in the comparison groups, they varied between 12.4 % (Schmucker and Losel 2013) and 27.4 % (Grossman et al. 1999). In the various meta-analyses the recidivism rates for the TG were approximately 1–10 percentage points lower than the rates for CG. Although, such differences may look small at first glance, one must take the relatively low sexual recidivism rates in the CG into account. For example, Hanson et al. (2002) reported an average sexual recidivism rate of 12.3 % for TG and 16.8 % for CG. This difference of 4.5 percentage points translates into a reduction of 27 % as compared to untreated offenders. The absolute difference between 9.0 % (TG) and 12.4 % (CG) in the meta-analysis of Schmucker and Losel (2013) was even smaller than in Hanson et al. (2002); however, the reduction in percent was the same (27 %). Of course, one must take into account undetected or unreported recidivism so that the “real” reoffending rates may be higher than those presented in Table 1. However, this is a general criminological problem that even may have decreased a bit in sexual offending because in many countries victims are more encouraged to report to the police or aid organizations.
Computing an overall ES from the various reviews is problematic because of the overlap between the reviews, different sample sizes, methods of analysis, and other issues. However, scanning the reported overall effect sizes across the different meta-analyses reveals that most of them are in the range of d = 0.10–0.30. Therefore d = 0.20 plus/minus 0.10 (approximately r ~0.10; odds ratio ~1.5) seems to be a realistic estimate of the effect that can be expected on average. This ES range of sexual offender treatment is similar to the ESs reported in the much more comprehensive research on general offender treatment (e.g., Losel 2012). It is noteworthy that sexual offenders do not only reoffend with sex offenses. In fact, the meta-analyses show that the recidivism rates of sexual offenders were higher for nonsexual offenses. For example, Hanson et al. (2009) reported 31.8 % (TG) versus 48.3 % (CG) and Schmucker and Losel (2013) reported 24.0 % (TG) versus 32.4 % (CG). This indicates that sexual offender treatment has a broader effect as well.
Treatment Characteristics As Moderators
Mode of Treatment. Nearly all meta-analyses show that cognitive-behavioral treatment (CBT) and relapse-prevention approaches (RP) exhibit larger effects than unspecific psychosocial or psychodynamic interventions. This result is in accordance with general offender treatment (Lipsey & Cullen 2007; Losel 2012). But although CBT is shown to be effective in principle, this program type does not guarantee reduced sexual reoffending. In well-controlled evaluations the effects of similar CBT programs ranged from strong positive over nearly zero to even negative effects (Schmucker and Losel 2013; see also individual studies in Hanson et al. 2009).
Beyond the evaluation of specific psychotherapeutic “schools,” the literature on “what works” in offender rehabilitation developed broader program characteristics such as the Risk-Need-Responsivity Model (Andrews et al. 2011). Similar to the findings from general offender treatment, Hanson et al. (2009) demonstrated that programs that fulfill all three principles are most successful for sexual offenders, while treatment that does not meet any of the three criteria even shows a slightly negative effect.
Those meta-analyses that also include hormonal therapy via antiandrogen medication and/ or surgical castration suggest relatively large effects for this kind of treatment. However, hormonal interventions are only indicated for a subgroup of offenders who are primarily motivated by sexual drive. Surgical castration is now rarely used because of legal and ethical reasons (Weinberger et al. 2005). The respective evaluation studies are of older date and they do not contain equivalent untreated groups. The respective CGs seem to be a negative selection of offenders not motivated for this kind of treatment or rejected by the decision committees. None of the studies reaches Level 3 of the MSMR (Losel and Schmucker 2005). Although the designs of hormonal medication evaluations are somewhat stronger, they also fail to meet the Level 3 eligibility criterion of Schmucker and Losel (2013). Furthermore, hormonal therapy has the highest refusal and dropout rates (e.g., Hall 1995). In these cases, those offenders who remained in treatment may have been a highly motivated selection. More sound evaluations of hormonal medication are necessary. One must also bear in mind that hormonal medication is rarely applied as a stand-alone measure but is normally combined with some form of psychosocial intervention. In that sense, these primary studies evaluated the effects of medication added to psychotherapeutic measures. Combinations of CBT and RP approaches with pharmacological treatment are promising for some groups of sex offender, and such approaches would be in accordance with common practice in other fields such as the treatment of depression.

Treatment Setting. Most meta-analyses report a tendency for larger effects in community than in custodial programs. However, some syntheses did not observe this difference (e.g., Alexander 1999; Hanson et al. 2002; Hanson et al. 2009). In principle, one would expect better effects of interventions in the community because treatment progress can be directly tested in risk situations, whereas the transfer of what has been learnt in custody is a key issue in resettlement and relapse prevention. However, the offender populations in both settings are not the same. No study compared treatment in institutional and ambulatory settings for the same type of sexual offenders. As more high-risk cases are to be expected in custody, the outcome differences between settings may be confounded with other features. When institutional treatment is further differentiated into prisons and forensic hospitals, some data suggest that the latter goes along with larger ES (Losel and Schmucker 2005; Schmucker and Losel 2013). In contrast, Alexander (1999) found larger ESs for prison compared with hospital settings, but this synthesis contains many methodologically weak studies.
Other Treatment Factors. In addition to treatment mode and setting, only a few other features of program delivery have been addressed in some meta-analyses. For example, Schmucker and Losel (2013) found that programs with a group format were less effective than programs that included individual sessions or were fully individualized. Although there are plausible arguments for treating sexual offenders in groups (Ware et al. 2009), this finding suggests that some differentiation according to specific offender needs is valuable (see also Marshall 2009).
Surprisingly little is known about the impact of the quality of program delivery. Only few primary studies report data on this issue so that it could not be addressed in the meta-analyses. Research in other areas of correctional treatment has shown that quality of delivery and program integrity are highly relevant for effectiveness (Goggin and Gendreau 2006). However, this issue needs to be investigated more systematically for sexual offender treatment, too. This also applies to the impact of therapist characteristics and the therapeutic relationship. Although research on general psychotherapy has shown that such features are as important as the treatment content, there is only little research on this issue in programs for sexual and other offenders.
Offender Characteristics As Moderators
Offense or Offender Types. The meta-analyses report only few differences in ES for different types of sexual offenses or offenders. For example, Gallagher et al. (2000) and Hall (1995) found no significant differences between various offense types. Alexander (1999) revealed larger ES for non-incest child molesters with male victims and the smallest ES for rapists. Losel and Schmucker (2005) reported significant effects for all offense categories except intra-familial child molesting. The unsatisfactory state of systematic knowledge about this issue is due to a lack of detailed diagnostic information in the primary evaluation studies.
Research on sex offender recidivism has shown that specific offender and offense characteristics such as use of violence, type of victims, general psychopathology, and paraphilia correlate with reoffending (Hanson and Morton-Bourgon 2005). However, most treatment studies differentiate only according to the index offense between child molesters, rapists, and exhibitionists or even use the summary characteristic of sex offender. Some narrative reviews suggest better success for CBT of child molesters and exhibitionists (e.g., Marshall et al. 1991), but the evidence is rather scarce and as yet there are no well-replicated results on differential indication from the treatment evaluations.
Risk Level. There is a clearer picture of findings with regard to offenders’ risk of sexual reoffending. Two recent meta-analyses showed that ESs are larger for groups at higher than lower risk (Hanson et al. 2009; Schmucker and Losel 2013). A simple explanation for this finding is that the base rate for sexual reoffending in low-risk groups is so low that even successful programs cannot further reduce them. In part, this finding may also be confounded with the age of offenders.
Age. According to the age-crime curve, young offenders have a higher risk of reoffending. Therefore, young age is included in evidence-based actuarial risk assessment instruments for sexual offenders. Although the present entry focuses on the treatment of adult offenders, some of the meta-analyses also included studies on juveniles. Losel and Schmucker (2005) and Schmucker and Losel (2013) found a tendency of larger ES in studies that addressed adolescents only. In contrast, Hanson et al. (2009) reported an opposite trend of larger ES in adult samples. Due to the small number of primary studies that specifically addressed adolescent sex offenders, the respective differences in all three meta-analyses did not reach statistical significance. However, two meta-analyses on the treatment of juvenile sexual offenders support the assumption of larger effects in these target groups: Walker et al. (2004) found a mean effect of d = 0.54 and Reitzel and Carbonell (2006) a mean of 0.47. With the exception of Gallagher et al. (2000), both ESs are clearly above those in the meta-analyses of mainly adult offenders (see Table 1).
Treatment Motivation. The motivation to engage in treatment and avoid reoffending is seen as a key factor for success. However, in contrast to classical psychotherapy treatment, motivation is no longer seen as an all-or-none category and a more or less static characteristic of the offender, but as a dynamic concept of interaction between the offender and his social context (McMurran 2002). Therefore, similar to interventions for drug-addicted patients, the treatment of sexual offenders is not only a voluntary offer. Recent findings support this view. Whereas Losel and Schmucker (2005) found a somewhat (but not significantly) larger effect in voluntary than in mandatory programs, Schmucker and Losel (2013) revealed nearly identical ESs for both approaches to treatment participation.
Methodological Features
Although practice is primarily interested in program and offender factors that moderate treatment effects, characteristics of the evaluation method are also very important. In the meta-analysis of Losel and Schmucker (2005), methodological characteristics of the primary studies even explained the largest amount of ES variation. However, in the field of sexual offender treatment, it is difficult to disentangle the independent influence of a factor because the subsamples with a specific characteristic are small and there are often confounded variables.
Design Quality. Table 1 suggests that the methodological quality varied substantially both within and between meta-analyses. In general it is still not satisfactory. The findings on the relation between design quality and the effect of sexual offender treatment are mixed. The two meta-analyses with a large portion of uncontrolled outcome studies showed the smallest effects (Alexander, 1999; Losel , 2000). The Gallagher et al. (2000) synthesis of studies with relatively sound designs reported the largest mean effect. However, the latter meta-analysis also contained studies that used not only official recidivism as outcome data but also self-reports, family reports, or other information. As these studies revealed relatively large effects, ES differences between meta-analyses do not necessarily depend on a single dimension of methodological rigor. The other meta-analyses on relatively sound studies revealed ESs that are lower. All three reviews found a mean ES at around 0.20 (Aos et al. 2001; Hanson et al. 2009; Schmucker and Losel 2013).
There is also no clear picture on this issue within the various meta-analyses. Some syntheses observed a tendency of lower ES in studies with weaker design (e.g., Gallagher et al. 2000; Polizzi et al. 1999). Others found an opposite tendency (Hanson et al. 2002, 2009) or no systematic relation between design quality and ES (Hall 1995; Losel and Schmucker 2005; Schmucker and Losel 2013). The same was the case with regard to RCTs versus other designs. In reviews on general offender treatment, there is also no clear relation between overall design quality and ES (Lipsey and Cullen 2007; Losel 2012). This finding deviates from studies on a broader range of criminological interventions where rigorous designs often go along with lower ES (Weisburd et al. 2001). However, multivariate analyses of the impact of methodological quality on the ES in sex offender treatment are hindered by lacking information and the small number of RCTs. The relation between ES and design quality may even depend on the use of a fixed versus random effects model of ES integration (e.g., Hanson et al. 2009). In some meta-analyses, results depended on whether a single study with extreme effects was included or not (e.g., Gallagher et al. 2000; Losel 2000).
Sample Size. The problem of disentangling moderators is also relevant with regard to sample size. Similar to findings on general offender treatment (Lipsey and Cullen 2007), some meta-analyses reported the largest effect in very small samples. This may be due to better program implementation in small studies, in particular when the evaluation was carried out in a demonstration project and the authors evaluated an own program. However, the impact of sample size could also reflect a publication bias because smaller studies require a larger ES to get a significant result. Accordingly, Gallagher et al. (2000) and Hanson et al. (2009) reported larger effects in published studies, however, the latter authors for the fixed effects model only. In contrast Hanson et al. (2002) found larger effects in unpublished studies and Losel and Schmucker (2005) even observed a somewhat greater moderator effect of sample size in unpublished studies.
Length of Follow-Up. Although the rate of recidivism increases with the length of follow-up, the ES in treatment evaluations seems not to decrease generally over time. For example, Losel and Schmucker (2005) and Schmucker and Losel (2013) found no significant correlation between ES and follow-up time. Gallagher et al. (2000) and Hall (1995) even reported that the length of follow-up related positively to ES. This contradicts results on general offender treatment (Lipsey and Cullen 2007) but may have been due to outliers with very long follow-up periods and very high ES. Very long periods of follow-up might also cause problems because data may have been erased from official registers for some (inactive) offenders.
Other Methodological Moderators. There are many other potential moderators of ES. However, they were not systematically addressed across the various meta-analyses. For example, Gallagher et al. (2000) and Losel and Schmucker (2005) found that official recidivism showed lower ESs than other outcome measures (i.e., self-reports or composite measures). Perhaps, official data are less sensitive to change but such effects are difficult to demonstrate due to confounding with other variables. Attrition rates also seem to be relevant for ES. High attrition rates may indicate a low quality of program implementation and also lead to lower effects when the dropouts are counted as part of the TG in an intent-to-treat analysis (Losel and Schmucker 2005).
A particularly important issue is the transparency of the report on the evaluation. Although the concept of descriptive validity (Losel and Koferl 1989) is not a characteristic of the evaluation process itself, it shows substantial correlations between r ¼ 0.24 and 0.50 with ES (Losel and Schmucker 2005; Schmucker and Losel 2013). It can be assumed that a detailed and transparent documentation of the treatment concept, implementation, outcome measurement, and statistical analysis indicates a good overall quality of the respective evaluation. Therefore, it is strongly recommended that program evaluations pay more attention to this issue.
Conclusions
This brief review of meta-analyses on the effects of sex offender treatment revealed an overall positive effect on sexual reoffending and various characteristics of the most promising interventions. However, the heterogeneity of study outcomes accompanied by a lack of detail in the documentation of programs, offender populations, setting variables, and other features as well as often weak study designs leaves many questions open. A further increase of high-quality primary studies and the systematic integration of their results are crucial to answer open questions and help turn suggestive findings into confirmed knowledge. Such studies should also focus on more homogeneous and well-assessed subgroups of sexual offenders and provide sound information on the treatment process. This would lead to a more solid and differentiated evidence base about what works for whom, under what conditions, in what contexts, and with regard to what outcomes. As sexual offending is a topic of much public concern, such evaluations are particularly important to replace stereotypes and opinions in policy making by sound evidence.
Bibliography:
- Alexander M (1999) Sexual offender treatment efficacy revisited. Sex Abus J Res Treat 11:101–116
- Andrews DA, Bonta J, Wormith S (2011) The risk-need-responsivity (RNR) model: does adding the Good Lives Model contribute to effective crime prevention? Crim Jus Behav 38:735–755
- Aos S, Phipps P, Barnoski R, Lieb R (2001) The comparative costs and benefits of programs to reduce crime. Version 4.0 (No. 01-05-1201). Washington State Institute for Public Policy, Washington
- Brooks-Gordon B, Bilby C, Wells H (2006) A systematic review of psychological interventions for sexual offenders I: randomised control trials. J Forensic Psychiatr Psychol 17:442–466
- Farrington DP, Gottfredson DC, Sherman LW, Welsh BC (2002) The Maryland scientific methods scale. In: Sherman LW, Farrington DP, Welsh BC, MacKenzie DL (eds) Evidence-based crime prevention. Routledge, London, pp 13–21
- Furby L, Weinrott MR, Blackshaw L (1989) Sex offender recidivism: a review. Psychol Bull 105:3–30
- Gallagher CA, Wilson DB, MacKenzie DL (2000) A meta-analysis of the effectiveness of sex offender treatment programs. Paper retrieved from http://www.wam.umd. edu/ wilsondb/papers/sexoffender.pdf
- Goggin C, Gendreau P (2006) The implementation and maintenance of quality services in offender rehabilitation programmes. In: Hollin C, Palmer E (eds) Offending behaviour programmes. Wiley, Chichester
- Grossman LS, Martis B, Fichtner CG (1999) Are sex offenders treatable? A research overview. Psychiatr Serv 50:349–361
- Hall GCN (1995) Sexual offender recidivism revisited: a meta-analysis of recent treatment studies. J Consult Clin Psychol 63:802–809
- Hanson RK, Gordon A, Harris AJR, Marques JK, Murphy WD, Quinsey VL, Seto MC (2002) First report of the collaborative outcome data project on the effectiveness of psychological treatment for sex offenders. Sex Abus J Res Treat 14:169–194
- Hanson RK, Morton-Bourgon KE (2005) The characteristics of persistent sexual offenders: a meta-analysis of recidivism studies. J Consult Clin Psychol 73:1154–1163
- Hanson RK, Bourgon G, Helmus L, Hodgson S (2009) The principles of effective correctional treatment also apply to sexual offenders: a meta-analysis. Crim Justice Behav 36:865–891
- Lipsey MW, Cullen FT (2007) The effectiveness of correctional rehabilitation: a review of systematic reviews. Ann Rev Law Soc Sci 3:297–320
- Losel F, Koferl P (1989) Evaluation research on correctional treatment in West Germany: a meta-analysis. In: Wegener H, Losel F Haisch J (eds) Criminal behavior and the justice system. Springer, New York pp 334–355
- Losel F (2000) The efficacy of sexual offender treatment: a brief review of German and international evaluations. In: van Koppen PJ, Roos N (eds) Rationality, information and progress in law and psychology. Metajuridica, Maastricht, pp 145–170
- Losel F, Schmucker M (2005) The effectiveness of treatment for sexual offenders: a comprehensive meta-analysis. J Exper Criminol 1:117–146
- Losel F (2007) Doing evaluation in criminology: balancing scientific and practical demands. In: King RD, Wincup E (eds) Doing research on crime and justice, 2nd edn. Oxford University Press, Oxford pp 141–170
- Losel F (2012) Offender treatment and rehabilitation: what works? In: Maguire M, Morgan R, Reiner R (eds) The Oxford handbook of criminology, 5th edn. Oxford University Press, Oxford, pp 986–1016
- Marshall WL (2009) Manualization: a blessing or a curse? J Sex Aggress 15:109–120
- Marshall WL, Marshall LE (2010) Can treatment be effective with sexual offenders or does it do harm? A response to Hanson (2010) and Rice (2010). Sex Offender Treat 5(2), online
- Marshall WL, Jones R, Ward T, Johnston P, Barbaree HE (1991) Treatment outcome with sex offenders. Clin Psychol Rev 11:465–485
- McGrath RJ, Cumming GF, Burchard BL, Zeoli S, Ellerby L (2010) Current practices and emerging trends in sexual abuse management: the Safer Society 2009 North American Survey. The Safer Society Press, Brandon
- McMurran M (2002) Motivation to change: selection criterion or treatment need? In: McMurran M (ed) Motivating offenders to change. Wiley, Chichester, pp 3–13
- Polizzi DM, MacKenzie DL, Hickman LJ (1999) What works in adult sex offender treatment? A review of prisonand non-prison-based treatment programs. J Offend Ther Comp Criminol 43: 357–374
- Reitzel LR, Carbonell JL (2006) The effectiveness of sexual offender treatment for juveniles as measured by recidivism: a meta-analysis. Sex Abus J Res Treat 18:401–421
- Schmucker M, Losel F (2008) Does sexual offender treatment work? A systematic review of outcome evaluations. Psicothema 20:10–19
- Schmucker M, Losel F (2013) Evaluating the effects of sexual offender treatment: an international meta-analysis of sound quality studies. Paper submitted for publication
- Walker DF, McGovern SK, Poey EL, Otis KE (2004) Treatment effectiveness for male adolescent sexual offenders: a meta-analysis and review. J Child Sex Abus 13:281–293
- Ware J, Mann RE, Wakeling HC (2009) Group versus individual treatment: what is the best modality for treating sexual offenders? Sex Abus Aust NZ 1:70–79
- Weinberger LE, Sreenivasan S, Garrick T, Osran H (2005) The impact of surgical castration on sexual recidivism risk among sexually violent predatory offenders. J Am Acad Psychiatr Law 33:16–36
- Weisburd D, Lum CM, Petrosino A (2001) Does research design affect study outcomes in criminal justice? Ann Am Acad Pol Soc Sci 578:50–70
- White P, Bradley C, Ferriter M, Hatzipetrou L (2009) Managements for people with disorders of sexual preference and for convicted sexual offenders [Cochrane Review]. The Cochrane Library (4). Oxford: Update Software
See also:
Free research papers are not written to satisfy your specific instructions. You can use our professional writing services to buy a custom research paper on any topic and get your high quality paper at affordable price.
ORDER HIGH QUALITY CUSTOM PAPER

Always on-time

Plagiarism-Free

100% Confidentiality

{kind=link}