
This sample Racism and Health Research Paper is published for educational and informational purposes only. If you need help writing your assignment, please use our research paper writing service and buy a paper on any topic at affordable price. Also check our tips on how to write a research paper, see the lists of health research paper topics, and browse research paper examples.
Introduction
Although racism appears to be an enduring feature of societies throughout the world, there is continuing debate about its origins. Some scholars find evidence of racism throughout recorded history, while others pinpoint its genesis in the fifteenth-century Enlightenment. Nevertheless, it is clear that the term racism itself was first coined in the early twentieth century, emerging as a critique of race relations in Western societies. Outside of academic circles the term was not in popular usage until the mid-twentieth century, with the concepts of institutional and internalized racism (discussed later) not appearing until the 1960s.
Given this history, it is not surprising that the extensive literature on ethnic/racial (hereafter ethnoracial) disparities in health produced in recent decades has, with few exceptions, failed to explicitly identify and study racism as a driver of these disparities. Although it has been shown that ethnoracial disparities in health are large and pervasive across health outcomes, as well as time and place, and that social exclusion/disadvantage are fundamental to such disparities (Nazroo and Williams, 2006), the overt study of racism as a driver of health inequality only began in earnest following an article by Krieger et al. (1993).
Since this time, a few hundred studies that overtly examine the relationship between racism and health have been published. Drawing in particular on recent scholarship by Paradies (2006a, b), this research paper begins by reviewing the conceptualization, operationalization, and characterization of racism as a determinant of health before examining the evidence from this small but burgeoning body of research and concluding with a discussion of limitations and future directions in the explicit study of racism and health. It should be noted that this research paper does not review the broader literature on ethnoracial disparities in health. Moreover, the burgeoning field of psychology that examines stereotyping, bias, and behavior in relation to different ethnic groups or races (hereafter ethnorace) is touched on only briefly.
Conceptualizing Racism
In conceptualizing racism as a determinant of health, it should first be recognized that racism is only one of several causes of ethnoracial disparities in health. Genetic, sociocultural, and socioeconomic differences between ethnoracial groups are also responsible for such disparities. While the latter two factors are substantial drivers of ethnoracial health disparities and are themselves strongly influenced by racism, genetic variation accounts for only a tiny fraction of health disparities across ethnoracial groups.
To the extent that racism drives health outcomes, it does so in interaction with other oppressions such as sexism, ageism, and classism. Oppression is manifested in societies through the unequal distribution of power among social groups resulting from attitudes, beliefs, behaviors, norms, and practices relating to these social groups. The phenomenon of oppression is also intrinsically linked to that of privilege. In addition to disadvantaging minority racial groups in society, racism also results in groups (such as Whites) being privileged and accruing social power.
Figure 1 is a representation of how privilege/oppression may act as a determinant of health. The processes shown in this figure occur across the dimensions of both time (history) and space (geography) as well as across the life course.
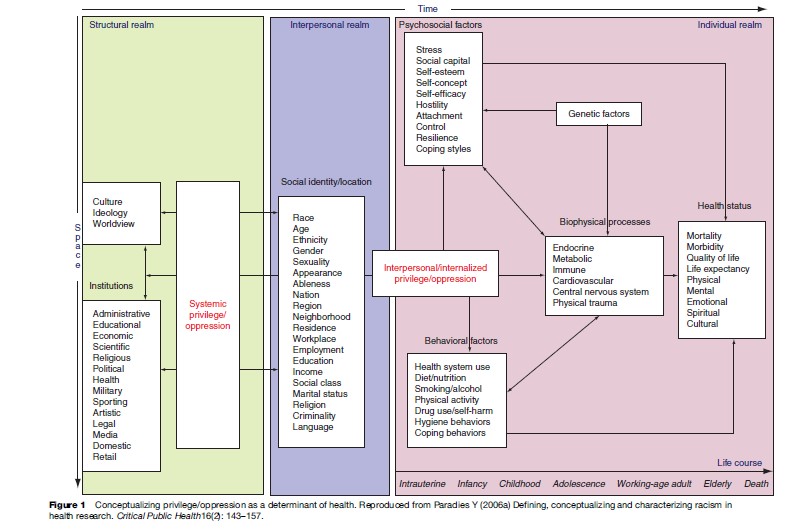
In the structural realm, fundamental features of society, as encapsulated by the terms culture, ideology, and worldview, interact with societal institutions and are influenced by and produce systemic privilege/oppression. Systemic privilege/oppression can be defined as the production, control, and access to material, information, and symbolic resources within a society that serve to increase power differentials between social groups. Systemic racism, which has also been referred to as institutional (or institutionalized), structural, cultural, societal, and civilizational racism, is an example of systemic privilege/oppression. As shown in Figure 1, systemic oppression acts to differentially construct and constrain the interpersonal realm as represented by an individual’s social identities (or locations). As a form of oppression, systemic racism is a strong determinant of an individual’s place of residence, living conditions, and socioeconomic position (SEP).
An individual’s social locations then become the basis on which interpersonal and internalized oppression is perpetrated. Interpersonal oppression is the interactions between individuals that serve to increase power differentials between social groups. Using the framework presented by Jones (2000), internalized oppression can be defined as the incorporation of attitudes, beliefs, or ideologies within an individual’s worldview that result in the unequal distribution of power among social groups. There are two forms – internalized dominance (i.e., privilege) and internalized oppression (i.e., oppression). Internalized dominance is the incorporation of attitudes, beliefs, or ideologies about the inferiority of other social groups and/or the superiority of one’s own social group. Conversely, internalized oppression is the incorporation of attitudes, beliefs, or ideologies about the superiority of other social groups and/or the inferiority of one’s own social group.
At the level of the individual, a biopsychosocial approach represents the interaction of interpersonal and internalized oppression with psychosocial and behavioral factors as well as biophysical (including genetic) processes. Individuals with various social identities who have disparate exposure to interpersonal and internalized oppression experience differential health outcomes by way of the processes shown. These processes also feed back into the interpersonal and structural realms, such that these three levels together enact on each other. The first step toward measuring the effects of racism, as represented in Figure 1, is to understand how racism can be operationalized as a determinant of health.
Operationalizing Racism
One of the most persistent difficulties in operationalizing the health effects of racism is the complexity involved in attributing a particular event to racism. Racism can be subtle, unintentional, unwitting and, in the case of internalized racism, even unconscious. Subjective experiences of racism may be caused by other forms of oppression, while experiences that are objectively racist may be attributed to other forms of oppression or to an individual’s own limitations. Moreover, some forms of systemic or internalized racism are frequently not perceived and may not be perceivable by those affected.
A more fundamental problem in attributing events to racism is that even the objective incidence of racism is an intrinsically relative phenomenon. That is, racism occurs when there are differential effects (in relation to power) by ethnorace. As such, any particular event is objectively racist only when it is clear that a different effect or outcome would have ensued in a situation that was identical except for the ethnorace of those involved. With the exception of carefully designed experimental studies, it is only possible to hypothetically consider such a counterfactual event, leaving an unavoidable degree of uncertainty in the attribution of an experience to racism.
Bearing these measurement difficulties in mind, there are two main approaches to operationalizing racism in health research: by indirect inference and as a direct perception or experience (i.e., perceived or self-reported racism). In the indirect approach to operationalizing racism, an association between racism and health is inferred by eliminating other possible explanations in design or analysis. A study using an indirect approach may, for example, conclude that Black–White health differentials that remain after adjustment for age, gender, sexuality, and SEP are due to experiences of racism. An indirect approach to studying racism is, generally, the only available option when racism is not perceivable or expressible by individuals or when racism cannot be readily or comprehensively measured – as is the case for some forms of systemic and internalized racism. Nonetheless, especially for observational studies, there are substantial methodological limitations to indirect approaches due to the possibility of incomplete coverage and poor measurement of confounders as well as an inability to investigate possible interactions between racism and other variables (see, however, Lauderdale, 2006 for a novel and sophisticated approach to addressing some of these limitations).
Direct approaches that involve the self-reporting of internalized, interpersonal, or systemic racism as an exposure, are the most commonly used in health research. Although the self-reporting of racism (as with any other attribute) is influenced by a range of psychological and sociodemographic factors (discussed later), this does not imply that the racism experienced and/or perceived and then reported by respondents is imagined, fabricated, or illusionary. In being measured primarily by way of self-reporting, racism is in no way unique among measures examined in public health research. Moreover, concepts such as self-assessed health status (which are inherently self-reported) have shown very strong and consistent associations with mortality and morbidity. Also, it is clear that along with similar concepts such as stress, self-reported perceptions/experiences of racism can affect health regardless of the objectivity of such reporting.
The Perception, Attribution, And Reporting Of Racism
In general, there are three possible factors to consider in the perception, attribution, and reporting of racism: (1) overestimation due to system blame, external attribution, or aspects of identity or social position/context that may lead to enhanced vigilance, hypersensitivity, etc.; (2) underestimation due to internalized racism, internal attribution, or aspects of identity or social position/ context that may preclude recognition or conscious awareness of racism (or produce skewed notions of fair treatment); and (3) cognitive/affective and methodological factors such as domain priming (i.e., the explicit use of race terminology) or social desirability bias that can either increase or decrease the perception, attribution, and reporting of racism.
In relation to overestimation, there is some evidence that a heightened sense of ethnoracial identity is associated with increased reporting of racism. However, this may only be the case for members of minority ethnoracial groups rather than for Whites and may occur only for ambiguous rather than blatant racist incidents. The relationship between reporting of racism and ethnoracial identity is bidirectional with many studies showing that minority ethnoracial group members who recognize more racism against their ethnoracial group have strengthened ethnoracial identification. Furthermore, a stronger identity may predispose individuals to experiencing (as well as perceiving and reporting) more racism through the way they interact with others. Although there has been far less research conducted on aspects of underestimation, there is preliminary evidence that internalized racism is associated with less perceived racism after adjustment for ethnoracial identity.
The explicit use of race terminology (rather than questions on discrimination in general which are later attributed to ethnorace) appears to increase reports of racism, perhaps by prompting respondents to assign racial meaning to ambiguous negative events. Another phenomenon that sheds light on the cognitive factors involved in reporting racism is the person–group discrimination discrepancy (PGDD). The PGDD describes the well-established tendency for individuals to report that their ethnoracial group is exposed to more racism than they are personally. There is evidence that the PGDD occurs when respondents determine the extent of personal discrimination through comparison with other members of their own ethnoracial group while determining the extent of group discrimination in comparison to other ethnoracial groups. The use of different standards of comparison (which may result in this ‘discrepancy’) raises broader questions about the cognitive processes involved in reporting racism.
Other research has demonstrated that self-reported racism is not related to neuroticism, hostility, cynicism, social desirability, or impression management. Conversely, reports of racism have been found to relate inversely to both self-deception (i.e,. a pervasive lack of insight) and self-affirmation. Moreover, as noted by Clark (2004), it is not known to what extent individuals habituate to experiences of racism and how this affects processes that may be related to health and well-being. In the context of such difficulties in operationalizing racism, the next section considers the ways in which racism can be characterized as a determinant of health.
Characterizing Racism
To date, the vast majority of research on racism and health has focused on perceived racism (and, more specifically, perceived racial discrimination). Figure 2 details the range of dimensions across which perceived racism has been characterized in health research, including dimensions of exposure to racism as well as possible reactions and responses to this exposure. As discussed previously, racism can be due to either oppression or privilege. However, virtually no research has been conducted in relation to racism as privilege and its association with health. As a result, the characterization of racism in Figure 2 (and as discussed later) relates only to the oppressive aspects of perceived racism.
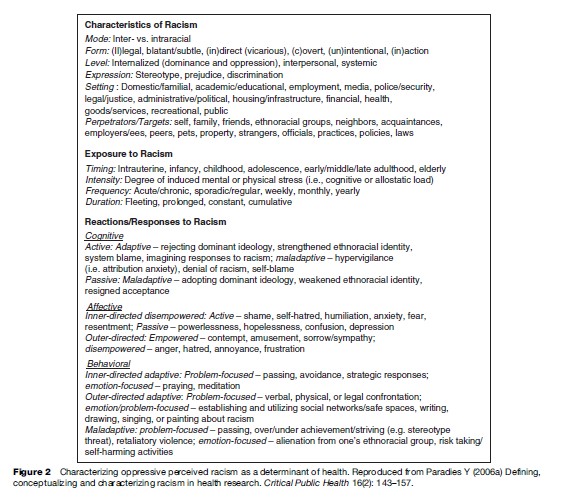
The characteristics of racism include its mode, form, level, expression, and setting as well as its perpetrators and targets. Racism can take a variety of forms including legal or illegal, direct or indirect, overt or covert, blatant or subtle, as well as vicarious by way of other targets of racism such as family or friends. Racism can also be unintentional as well as intentional and may occur through both action and inaction.
Some scholars contend that racism can occur between individuals of the same ethnorace (intraracially) as well as between individuals of different ethnoraces (interracially). However, there is continuing debate in this field as to whether intraracial racism should be accepted as a form of racism. Although some argue that members of minority ethnoracial groups lack the power to be racist, it is well established that minority group members discriminate against each other on the basis of racial characteristics such as skin color, and it is probable that such behavior affects the social power of those targeted. While very little research has examined intraracial racism, there is preliminary evidence of its deleterious effect on health.
Racism can be expressed through stereotypes, prejudice, or discrimination – that is, racist beliefs (cognition), emotions (affect), and behaviors, respectively – in a range of settings that correspond to the institutions represented in the structural realm of Figure 1. There is also a range of possible perpetrators or targets of racism, some of which are shown in Figure 2. Exposure to racism can occur at different stages of the life course with varying frequency at a range of intensities in relation to mental or physical stress. The duration of exposure to racism can also vary from fleeting to constant and can occur cumulatively across settings or over time.
Reactions/responses to racism may be cognitive, affective, or behavioral and in active or passive as well as adaptive or maladaptive forms. Self-blame is a cognitive, active, maladaptive response that occurs when a racist experience is given an internal attribution by an individual (i.e., through self-blame). In contrast, the cognitive, active, adaptive response of system-blame occurs when a racist experience is given an attribution external to the self. Another cognitive, maladaptive, active response to racism is hypervigilance in which an individual devotes an extreme amount of cognitive effort to anticipating racism, attempting to prevent racism, or in determining whether racism has occurred. This coping response can result in additional stress above and beyond the direct effects of racism itself. ‘Denial of racism’ and ‘self-blame’ (active responses) and ‘resigned acceptance’ (passive response) are cognitive responses that negate the need to process experiences of racism at all.

Affective or emotional responses to racism can be classified as either inner-directed or outer-directed. Inner-directed, disempowered, affective responses can be either active (e.g., shame, self-hatred, humiliation, anxiety, fear, resentment) or passive (e.g., powerlessness, hopelessness, confusion, depression), while outer directed, emotional responses, which are by definition active, can be either empowered or disempowered. Empowered responses occur when an individual who experiences racism projects inferiority onto the perpetrator and feels contempt, amusement, and/or sorrow or sympathy for them, while disempowered responses involve emotions such as anger, hatred, annoyance, or frustration.
Behavioral responses to racism can either be adaptive or maladaptive and within these categories can be problem or emotion-focused. As with affective responses, adaptive behavioral responses can be inner or outer-directed. Inner-directed, problem-focused, adaptive responses include avoiding situations in which racism is likely to occur as well as strategic decisions not to respond to racism. Inner-directed, emotion-focused, adaptive responses include contemplative/relaxing techniques such as praying and meditation, while outer-directed, adaptive, behavioral responses include the exclusively problem-focused approach of confronting the perpetrator(s) as well as establishing and/or using social networks and expressing/discussing racist experiences, which can act as either problem or emotion-focused approaches, depending on the situation in question.
Overand underachievement or striving are maladaptive, problem-focused, behavioral responses to racism. The phenomenon of ‘stereotype threat’ is an example of underachievement that occurs when a negative stereotype about one’s ethnorace causes self-stigmatization and reduced performance in an activity or situation. Retaliatory violence after experiencing racism is also an example of a maladaptive, problem-focused, behavioral response. Emotion-focused, maladaptive, behavioral responses include alienation from one’s ethnoracial group members and risk-taking and/or self-harming activities.
Finally, ‘passing’ is a problem-focused response, available to some people in some contexts, in which an individual’s ethnoracial identity is either not deployed, or is denied to avoid racism. Passing can be either adaptive or maladaptive with the short-term benefit of avoiding racist situations but long-term risk of weakening ethnoracial identity and social isolation from one’s ethnoracial group.
Racism, Health, And Well-Being
Having detailed how the oppressive aspects of perceived racism have been explicitly studied in public health, we can now turn to a discussion of findings from this recent body of research, which focus primarily on perceived racial discrimination. First, however, let us consider the smaller body of research that has explicitly examined racism using indirect methods. This research has focused primarily on racial discrimination in health care as well as residential segregation.
Indirect Studies OF Racism
It is undeniable that the most pernicious effects of racism on health are exerted through institutional mechanisms that are difficult to measure in standard epidemiological studies. Residential racial segregation that refers to the physical separation of ethnoraces in different residential areas is one example of such an institutionalized mechanism. Historically, the dominant group in many racialized societies has restricted the areas in which nondominant groups could reside. In countries like the United States and South Africa, residential segregation has persisted long after the legal codes supporting them were repealed.
Research from the United States reveals that residential segregation is a neglected but enduring legacy of racism that adversely affects the health of African-Americans in multiple ways. Residential segregation restricts access to education and employment opportunities and is a central mechanism by which racial differences in SEP have been created and reinforced. Accordingly, all indicators of SEP are strongly patterned by ethnorace, and ethnoracial differences in SEP contribute to ethnoracial disparities in health.
Segregation also results in unhealthy physical and social environments for minority ethnoracial groups through either the poor quality or high cost of nutritious foods, a lack of appropriate recreational facilities, exposure to toxic environmental substances, a high level of criminal victimization, and more retail outlets for (and excessive marketing of ) alcohol and tobacco. Medical care is also of poorer quality in segregated areas, with segregation contributing to racial disparities in preventive, screening, diagnostic, treatment, and rehabilitation services. Furthermore, the concentrated poverty and cumulative disadvantage of segregated neighborhoods can result in increased exposure to chronic stressors.
U.S. research indicates that due to residential segregation, the worst urban residential conditions for Whites are superior to the average residential conditions for Blacks. Several empirical studies have also found that highly segregated areas have higher rates of infant and adult mortality, as well as certain chronic and infectious diseases.
In relation to health care specifically, recent research has demonstrated that despite presenting with the same clinical indications and being treated at the same healthcare institution with the same health insurance coverage, members of ethnoracial minorities are less likely to receive appropriate medical care (e.g., cardiovascular, renal, and general surgical procedures) than members of dominant groups such as Whites (see, e.g., Smedley et al., 2003). Furthermore, research has found that health providers contribute to this systemic racism by way of clinical decisions that are influenced by both explicit (Van Ryn et al., 2006) and implicit (Green et al., 2007) racist perceptions of minority ethnoracial groups. This is an emerging area of research and further work is required to determine what contribution racism makes to ethnoracial differentials in medical care.
Direct Studies Of Racism
A recent review by Paradies (2006b) demonstrated a strong association between self-reported racism and ill health after adjustment for a range of confounders. Evidence from longitudinal studies also suggests that selfreported racism precedes ill health rather than vice versa. Furthermore, the few dozen studies of racism and health that have included both black and white populations demonstrate that self-reported racism accounts for some of the Black–White disparity in health outcomes.
The most consistent finding in this body of research is the association between racism and mental (ill) health such as psychological distress, depression, and anxiety. Racism also appears to be consistently associated with maladaptive behaviors such as smoking, alcohol, and substance misuse. Although racism has been associated with objectively measured physical health outcomes such as low birth weight and hypertension, the overall evidence for an association between self-reported racism and physical health is more equivocal than the concomitant association with mental health.
There are a number of reasons that could explain why self-reported racism is more strongly associated with mental rather than physical health. Because most research in this area has measured health via self-report, it is possible that the association between racism and mental ill health is exaggerated due to biases arising from the self-reporting of both exposure and outcome (Paradies, 2006b). If not caused by measurement artifice, the relatively weaker association between racism and physical health may be due to a delayed effect of racism on physical health that is mediated by mental ill health. However, we are aware of no longitudinal studies that could shed light on this possibility as no such studies, to our knowledge, have examined the interactions between mental and physical health outcomes and self-reported racism.
Future Directions
The relatively stronger association between self-reported racism and mental health outcomes raises questions about the mechanisms by which racism affects health. It is currently unclear what combination of pathopsychological effects on the mind and/or direct or indirect (i.e., through other body systems) neurophysiological changes mediate the association between self-reported racism and ill health. As suggested by Harrell et al. (2003) and Mays et al. (2007), studies that employ pharmacological blocks and functional neuroscience approaches may shed light on the psychophysiology of racism. Researchers in the field of stress are now examining biomarkers specific to body systems (i.e., cardiovascular, neuroendocrine, immune) with evidence emerging that particular stressors differentially affect physiological systems. Evidence that racism is more strongly associated with diastolic, than systolic, blood pressure is an example of such specificity. Clearly, further physiological research on racism is required to uncover the biological processes through which this phenomenon affects health. Moreover, the continuing debate on whether racism is a form of stress or a construct separate from stress (with evidence that stress both mediates and moderates the relationship between racism and health), may also be resolved through such psychophysiological research.
Other than preliminary evidence that a heightened sense of ethnoracial identity attenuates the adverse effects of self-reported racism on health, there has been limited research on moderation/mediation of the relationship between racism and health. Similarly, other than some evidence that the active coping is associated with better health outcomes than passive coping, little is known about the efficacy of various responses/reactions to racism in relation to health.
There has also been a scarcity of research on the health effects of racism across ethnoracial groups, with most studies focusing only on African-Americans. Even among studies that do consider racism across ethnoracial groups, it is common to statistically adjust for ethnorace rather than undertake stratified analyses. More nuanced analysis will be required to understand the degree to which associations between self-reported racism and health vary across ethnoracial groups. As part of such research, the privileging aspects of racism for dominant ethnoracial groups (e.g., Whites) could also be investigated and further examination of intraracial racism may resolve the continuing conceptual debate centered on this phenomenon.
Future research in this field of study is also required to characterize the multiple pathways through which institutionalized racism affects health. Furthermore, despite evidence of an association with ill health, limited attention has been focused on internalized racism. Work is needed to identify the best approach to assessing this phenomenon and to determine its impact on population health.
A significant limitation in this field is that direct approaches to studying racism have relied too heavily on single-item and unvalidated measures of self-reported racism, which are of limited utility (Paradies, 2006b). There are, however, three instruments that have been commonly used to assess self-reported racism in this field: the Everyday Discrimination Scale (Williams et al., 1997), Experiences of
Discrimination scale (Krieger et al., 2005) and the Schedule of Racist Events (Landrine et al., 2006). Given that these instruments have been subjected to psychometric validation and are able to assess different types of oppression across a range of ethnoracial groups, future research should (where possible) use these instruments rather than developing measures de novo.
Only a minority of direct studies of racism have specified a time frame over which exposure to racism should be reported by respondents and there is ongoing debate on the appropriateness of specifying time frames for self-reported racism. Utsey and Ponterotto (1996) have argued that an unspecified time frame is appropriate given the long-lasting nature of racist experiences. However, it is unclear whether respondents report recent and/or highly salient/traumatic experiences of racism when responding to questions without a specified time frame. Also, Blank et al. (2004) have noted that the inclusion of an explicit time frame on surveys is necessary to estimate the rate of exposure and to avoid confounding time-series analyses. By measuring self-reported racism with and without specified time frames in the same study, as well as investigating diary methods that capture events as they occur (Hill et al., 2004), future research will be able to shed light on this unresolved issue.
Most research in this emerging field has assessed self-reported interpersonal racism. As such, further research on internalized racism, vicarious racism (racism experienced by family or friends), systemic racism, and setting-specific racism (e.g., racism in the workplace) is warranted. Psychological research into the factors affecting perception, attribution, and reporting of racism (including the interplay between objective and subjective racism) is also required, especially studies that can uncover the factors affecting respondents’ retrospective estimate of racism exposure across a range of settings, contexts, and time frames.
Measuring exposure to racism in its full complexity requires attention not only to racist incidents over the life course, but also to the potential intergenerational effects of racism. Historical trauma is the cumulative psychological wounding of an individual and his/her ethnoracial group due to a history of genocide and oppression. The importance of assessing this dimension of racism is highlighted by recent research on the health effects of historical and transgenerational trauma in relation to American Indians and Indigenous Australians, respectively. Assessment instruments with good psychometric properties have been developed to assess historical trauma and have found, for example, that some 50% of American Indians think regularly about these historical losses. Empirical studies have also linked exposure to historical trauma to multiple poor health outcomes, emphasizing the need for further research on this aspect of racism.
The study of racism and health is a newly emerging area of study in public health. It is clear that conceptual clarity and rigorous, theoretically based empirical research will be required to both unravel the complex pathways through which racism acts as a determinant of health and to help address the deleterious effect of racism on health and well-being.
Bibliography:
- Blank R, Dabady M, and Citro C (2004) Measuring Racial Discrimination. Washington, DC: National Academies Press.
- Clark R (2004) Significance of perceived racism: Toward understanding ethnic-group disparities in health, the later years. In: Anderson NB, Bulatao RA, and Cohen B (eds.) Critical Perspectives on Racial and Ethnic Differences in Health in Late Life, pp. 540–566. Washington, DC: National Academy Press.
- Green AR, Carney DR, Pallin DJ, et al. (2007) Implicit bias among physicians and its prediction of thrombolysis decisions for black and white patients. Journal of General Internal Medicine 22(9): 1231–1238.
- Harrell JP, Hall S, and Taliaferro J (2003) Physiological responses to racism and discrimination: an assessment of the evidence. American Journal of Public Health 93(2): 243–248.
- Hill CV, Neighbors HW, and Gayle HD (2004) The relationship between racial discrimination and health for Black Americans: measurement challenges and the realities of coping. African American Research Perspectives 10: 89–98.
- Jones CP (2000) Levels of racism: A theoretic framework and a gardener’s tale. American Journal of Public Health 90(8): 1212–1215.
- Krieger N, Rowley D, Hermann AA, Avery B, and Phillips MT (1993) Racism, sexism and social class: implications for studies of health, disease, and well-being. American Journal of Preventive Medicine 9(6): 82–122.
- Krieger N, Smith K, Naishadham D, Hartman C, and Barbeau EM (2005) Experiences of discrimination: validity and reliability of a self-report measure for population health research on racism and health. Social Science and Medicine 61(7): 1576–1596.
- Landrine H, Klonoff EA, Corral I, Fernandez S, and Roesch S (2006) Conceptualizing and measuring ethnic discrimination in health research. Journal of Behavioral Medicine 10: 1–16.
- Lauderdale DS (2006) Birth Outcomes for Arabic-named Women in California Before and After September 11. Demography 43(1): 185–201.
- Mays VM, Cochran SD, and Barnes NW (2007) Race, race-based discrimination, and health outcomes among African Americans. Annual Review of Psychology 58: 201–225.
- Nazroo JY and Williams DR (2006) The Social Determination of Ethnic/ Racial Inequalities in Health. In: Marmot M and Wilkinson RG (eds.) Social Determinants of Health, 2nd edn., pp. 238–266. Oxford, UK: Oxford University Press.
- Paradies Y (2006a) Defining, conceptualizing and characterizing racism in health research. Critical Public Health 16(2): 143–157.
- Paradies Y (2006b) A systematic review of empirical research on self-reported racism and health. International Journal of Epidemiology 35(4): 888–901.
- Smedley BD, Stith AY, and Nelson AR (2003) Unequal treatment: confronting racial and ethnic disparities in health care. Washington, DC: National Academy Press.
- Utsey SO and Ponterotto JG (1996) Development and validation of the index of race-related stress (IRRS). Journal of Counseling Psychology 43(4): 490–501.
- Van Ryn M, Burgess D, Malat J, and Griffin J (2006) Physicians’ perceptions of patients’ social and behavioral characteristics and race disparities in treatment recommendations for men with coronary artery disease. American Journal of Public Health 96(2): 351–357.
- Williams DR, Yu Y, Jackson JS, and Anderson NB (1997) Racial differences in physical and mental health: socioeconomic status, stress, and discrimination. Journal of Health Psychology 2(3): 335–351.
- Atkinson J (2002) Trauma Trails, Recreating Songlines: The Transgenerational Effects of Trauma in Indigenous Australia. Melbourne, Australia: Spinifex Press.
- Brown TN (2001) Measuring self-perceived racial and ethnic discrimination in social surveys. Sociological Spectrum 21: 377–392.
- Branscombe NR, Schmitt MT, and Harvey RD (1999) Perceiving pervasive discrimination among African Americans: Implications for group identification and well-being. Journal of Personality and Social Psychology 77(1): 135–149.
- Clark R, Anderson NB, Clark VR, and Williams DR (1999) Racism as a stressor for African Americans: a biopsychosocial model. American Psychologist 54(10): 805–816.
- Cutler DM, Glaeser EL, and Vigdor JL (1997) Are Ghettos Good or Bad? Quarterly Journal of Economics 112(3): 827–872.
- Harrell SP (2000) A multidimensional conceptualization of racism-related stress: implications for the well-being of people of color. American Journal of Orthopsychiatry 70(1): 42–57.
- Hill CV, Njai RS, Neighbors H, Williams-Flournoy DF, and Jackson JS (2003) Racial discrimination and the physical health of Black Americans: A review of the literature on community studies of race and health. African American Research Perspectives 9(1): 10–23.
- Krieger N (1999) Embodying inequality: a review of concepts, measures, and methods for studying health consequences of discrimination. International Journal of Health Services 29(2): 295–352.
- Major B, Quinton WI, and McCoy SK (2002) Antecedents and consequences of attribution to discrimination: theoretical and empirical advances. Advances in Experimental Social Psychology 34: 251–330.
- Sechrist GB, Swim JK, and Stangor C (2004) When do the stigmatized make attributions to discrimination occurring to the self and others? The roles of self-presentation and need for control. Journal of Personality and Social Psychology 87(1): 111–122.
- Sellers RM and Shelton JN (2003) The role of racial identity in perceived racial discrimination. Journal of Personality and Social Psychology 84 (5): 1079–1092.
- Whitbeck LB, Adams GW, Hoyt DR, and Chen X (2004) Conceptualizing and measuring historical trauma among American Indian people. American Journal of Community Psychology 33(3/4): 119–130.
- Williams DR and Collins C (2001) Racial residential segregation: a fundamental cause of racial disparities in health. Public Health Reports 116(5): 404–416.
- Williams DR, Neighbors HW, and Jackson JS (2003) Racial/ethnic discrimination and health: findings from community studies. American Journal of Public Health 93(2): 200–208.
See also:
Free research papers are not written to satisfy your specific instructions. You can use our professional writing services to buy a custom research paper on any topic and get your high quality paper at affordable price.
ORDER HIGH QUALITY CUSTOM PAPER

Always on-time

Plagiarism-Free

100% Confidentiality


