
This sample Sports Injuries Research Paper is published for educational and informational purposes only. If you need help writing your assignment, please use our research paper writing service and buy a paper on any topic at affordable price. Also check our tips on how to write a research paper, see the lists of health research paper topics, and browse research paper examples.
Sports Injury As An International Public Health Issue
Participation in sport is encouraged by government agencies and physical activity experts because participation provides health, physical, mental, social, and economic benefits to the individual and the community. There are many reasons individuals choose to participate in sport, including fitness, general health benefits, social interaction, and competition. However, an increased level of participation in sport increases exposure to the hazards and risks associated with injury. There is a broad spectrum of sports injuries, ranging from minor injuries such as grazes and bruises through moderate injuries such as sprains, strains, and contusions to severe injuries such as fractures, concussion, and very rarely, death.
While participation in sport is a universal goal, sports injury is generally not regarded as a priority area internationally within the area of injury prevention and control, because such injuries rarely lead to death. However, at least in developed countries, when the total burden of injury has been quantified, sports injury has been shown to be a significant contributor to and one of the major causes of injury-related morbidity. There is also a substantial economic burden associated with sports injuries for both individuals and society with respect to the duration and nature of treatment, the amount of sport and/or working time lost, permanent damage or disability, reduced quality of life, and other monetary costs. It has been reported that approximately one-third of all sport and active recreation injuries affect activities of daily living and/or have adverse effects on participation or performance in subsequent activity (Finch and Cassell, 2006). Sports injuries, therefore, have the potential to significantly contribute to future ill health through their longer-term consequences of nonparticipation in physical activity and increased risk of chronic musculoskeletal conditions, including osteoarthritis.
Epidemiology Of Sports Injury
Although sports injury has been identified as a priority area by some local and national government agencies, there is limited information on the incidence of sports injury at the broad community level in most countries. This is because there are few comprehensive national or even local routine data collection systems in place to monitor sports injuries. The main sources of routinely collected population-based sports injury data are general health statistics collections, such as those relating to hospital admissions, emergency department presentations, and coronial records. These data are usually only available in developed countries and there is no population-based information available for developing countries. However, this information represents only the tip of the iceberg with respect to the true burden of sports injuries as fewer than 30% of all sports injuries receive treatment at a hospital setting. For example, in Australia it has been estimated that for every sports injury requiring hospital admission, 10 cases are treated at hospital emergency departments, 12 are treated by general practitioners, 41 are treated by other medical or allied health professionals, and 145 receive no treatment (Cassell et al., 2003). Additionally, it is difficult to describe the rate of sports injury relative to other injuries, as many population-based surveillance systems that are used to report injury hospitalizations and deaths do not have sufficient codes to clearly identify sports injury cases.
However, some international statistics that are available emphasize the burden associated with sports injury. Studies in the United States have estimated that 4.3 million nonfatal sport and recreational injuries are treated in hospital emergency departments each year, comprising 16% of all unintentional injury-related emergency department visits (Centers for Disease Control and Prevention, 2002) and that the rate of unintentional sports and recreational injuries is 332.5 persons per 100 000 population (Conn et al., 2006). Over a 12-month period, there were 45 452 sport/leisurerelated hospitalizations across Australia, accounting for 0.7% of all hospitalizations and corresponding to an injury incidence of 231.4 hospitalizations per 100 000 population (Flood and Harrison, 2004). The vast majority of sport and recreation-related hospitalizations occur in males (73.9%) and the greatest number of hospitalized injuries are sustained by those aged 0–14 years. In Germany, 3.1% of adults sustain a sports injury each year, ranking sports injuries as the second most common type of injury after domestic accidents, with nearly two-thirds of these sports injuries resulting in time taken off work (Schneider et al., 2006). A survey conducted with children and adolescents in Switzerland reported a much higher injury rate, with 28.2% of girls and 35.9% of boys reporting one or more sports injuries per year, with 2.1% of girls and 6.5% of boys reporting at least one hsopitalization due to a sports injury (Michaud et al., 2001). Other studies have investigated the costs of injury, and sports injury ranks highly compared with other types of injury. In one study, most injuries were associated with participation in sport and leisure activities (40.2%), followed by work (11%) and transportation (10.8%) (Watson and Ozanne-Smith, 1998). Another study reported that in 1998–99, the total cost of sports injuries in one Australian state was AU$92 million (Potter Forbes and Aisbett, 2003). This was comprised of AU$40 million for direct costs and AU$52 million for mortality and morbidity costs (Potter Forbes and Aisbett, 2003). Sports injury ranked only seventh in terms of lifetime cost, but third in terms of direct cost (AU$40 million) after falls (AU$333 million) and road traffic accidents (AU$62 million). Interestingly, when considering the risk of sports injury from an occupational perspective, an English study found that the risk of injury in professional football (soccer) is around 1000 times greater than the risk observed in other industrial occupations, such as construction and mining (Hawkins and Fuller, 1999). These international statistics reemphasize the burden associated with sports injury.
In developing countries, although sports are a common pastime, the extent of sports injury is not known. Developing countries often have a unique range of challenges relating to sports injury prevention, such as a lack of available safety equipment (such as helmets and basic items such as shoes), poor playing equipment and surfaces (such as playing on grounds that have dangerous items such as glass) and few coaches with appropriate training, qualifications and understanding of sports injury prevention. For developing nations with limited resources, the focus has often been on other injury concerns, such as road trauma, violence, and drowning. It has also been difficult to determine the true extent of the sports injury problem across the globe as injury surveillance systems have often adopted differing definitions of ‘sport’ and ‘injury.’ While some studies have incorporated informal active recreation, physical activity, and leisure and play activities, others have examined only more formal, competitive sport. With respect to the definition of injury, a major limitation in the sports injury literature is that there is no common operational definition of injury, and it has varied according to the source of the injury data and the purpose of the injury surveillance. When comparing the results reported in sports injury studies (e.g., injury incidence rates), it is therefore important to consider how the definition of injury used in each study has affected the results obtained. A significant recent advance has been the development and publication of consensus definitions of injury in particular sports, including cricket (Orchard et al., 2005) and football (soccer) (Fuller et al., 2006), and of particular injury types, such as concussion (McCrory et al., 2005). Another data limitation for the general area is that exposure-adjusted sports injury rates have not been widely reported internationally, and this has hampered efforts at fully describing the sports injury problem.
Categories Of Sports Injuries
Sports injury can occur to almost any structure or tissue of the body, particularly bone, cartilage, tendon, ligament, muscle, and brain. Two broad categories of sports injury have been reported in the literature according to the nature of the event(s) leading to their occurrence. Acute injuries occur suddenly and are associated with a single, macrotraumatic event. The inciting event, or mechanism of the injury, is usually clearly identified as being the application of some external force with resultant tissue disruption. Examples of acute injuries are fractures and ligament sprains as the result of collisions or tackling in sport, awkward landings, or falls. The second category is often referred to as ‘overuse’ injury, with terms such as ‘gradual onset,’ ‘chronic,’ ‘idiopathic,’ and ‘repetitive microtrauma’ sometimes used. These injuries develop gradually and are associated with repetitive microtrauma of the musculoskeletal system, in which a number of repetitive forces, each lower than the critical limit of selected tissues, produce a combined fatigue effect over time and reduce the tolerance of the affected structures to load. The event causing the injury is not as apparent as is the case in acute injuries, and the damage to the tissues is more a result of mechanical degradation than of acute disruption. Examples of overuse injuries are stress fractures and tendonitis, which can be associated with factors such as excessive training or running repeatedly on very hard surfaces.
Different sports generally have diverse injury profiles because of the unique playing and movement demands. Therefore, the nature of injury, as well as the body site affected, can differ substantially across sports. In contact sports such as rugby football, the majority of injuries are caused by tackles (collisions) with other players, resulting in contusions, dislocations, lacerations, and inflammation to the head, trunk, and upper and lower limbs. For sports characterized by sudden changes of movement, including hockey and basketball, there are a substantial number of lower limb sprains and strains. In contrast, for noncontact sports, such as tennis or running, a large burden can be associated with overuse injuries, including rotator cuff tendonitis, epicondylitis, and shin splints. The injuries sustained by different players within a given sport can also vary widely according to the position that they play and the phase of play. For example, the injuries sustained by a baseball pitcher (e.g., an overuse injury to the elbow) are quite different from the injuries sustained by a batter (e.g., a fractured finger caused by being hit by the ball).
As described earlier, the data available regarding sports injuries differ according to the methods by which they have been collected and reported. A consistent finding across those studies that have used hospital admissions data is that the sports injury most often admitted to hospital is a fracture to the upper or lower limb, with head and spine injuries also being treated frequently in this setting. With respect to emergency department presentations, the majority of injuries are sprains and strains of the upper and lower limbs, as well as fractures. Cuts, lacerations, bruises, and hematomas are injuries treated frequently in emergency departments. Similarly, the injuries most frequently presenting to general practitioners are sprains, strains, bruises, and hematomas. It is likely that the majority of overuse injuries sustained in sports are treated by allied health professionals, such as physiotherapists and chiropractors; however population-based data are scant in this area, with the majority of studies being limited to participants of specific sporting groups.
Sports Injury Risk Factors
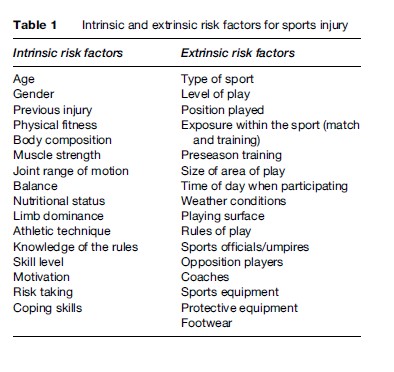
Risk factors for sports injury can be divided into two main categories (Table 1): intrinsic (internal, personal) and extrinsic (external, environmental; van Mechelen et al., 1992; Meeuwisse, 1994). Intrinsic and extrinsic injury risk factors can also be classified as being modifiable or nonmodifiable (Bahr and Holme, 2003). While nonmodifiable factors such as age, gender, and injury history may be important, it is imperative that the primary focus be on those factors that are potentially modifiable through interventions in physical training or behavior, including flexibility, strength, and training volume (Bahr and Holme, 2003). It is important to note that the cause of sports injury is multifactorial, and injury results from the interaction of a number of risk factors and events (Meeuwisse, 1994). Injuries are often attributable, not to the presence of a single extrinsic or intrinsic risk factor, but to combinations of these risk factors.

The four most consistently identified risk factors for injury across a range of sports, to date, are gender, age, previous injury, and exposure. Males have been identified as having a rate of injury two to three times greater than that of females. This may reflect a difference in the sports chosen by males and females, with males participating more frequently in higher-risk activities, including contact sports like football. Males may also adopt more aggressive behavior, placing them at a higher risk of injury. With respect to age, generally those in the 15–49 age group have a much higher rate of injury, followed by children younger than 15 years (Finch and Cassell, 2006). As with the difference in injury rates according to gender, the reason that young people may be at increased risk could be the types of activities in which they participate, as well as the physical differences between adults on one hand and children and adolescents on the other. Previous injury may contribute to high injury risk due to increased susceptibility of the tissues of the body due to incomplete rehabilitation or inadequate preparation. Finally, inappropriate exposure to a sport (too much or too little) is detrimental to the tissues of the body through overuse or inadequate preparation for sports participation.
The majority of research that has investigated potential risk factors for sports injury to date has focused on specific sports, particular subgroups of participants, certain playing positions, and/or particular injury diagnoses. In addition, many studies have included only elite-level participants. However, on a frequency basis, most injuries occur to community-level participants as they account for the vast majority of all participants. Nevertheless, the elite or professional sports studies have provided valuable information that can be used to inform the development of injury prevention efforts and establish the priority areas for continued investigation.
Most of the information about sports injury available relates to adult participants, and often injury prevention strategies, programs, and recommendations that are designed for adults are simply extrapolated to adolescents and children. However, it must be recognized that children are not just small adults, and it is essential that continued actions specifically recognize the risk factors for sports injury to young participants so that appropriate injury prevention strategies can be developed.
Sports Most Commonly Associated With Injury
In general, participation in team ball sports, such as hockey, football (soccer, rugby league, rugby union, Australian football, American football), basketball, handball, baseball, softball, cricket, and netball is associated with an increased risk of injury in comparison with individual sporting activities. The risk tends to be substantially higher for the contact sports. However, there are exceptions to this, with activities including horse riding, motorsports, cycling, waterskiing, and downhill skiing being associated with an increased rate of injury.
Sports Injury Prevention
Although it has been acknowledged that most sports injuries could be prevented or controlled, traditionally the main focus of the health and funding sectors has been on the diagnosis, treatment, and rehabilitation of sports injury, rather than on prevention. To ensure the maximal safety of sports participants, it is necessary to focus on the prevention of sports injuries, with the development of successful sports injury prevention strategies that rest on a solid evidence base. Several conceptual frameworks relating to sports injury prevention have been proposed. The most recent is the six-stage Translating Research into Injury Prevention Practice conceptual framework, which provides the theoretical underpinning for all sports injury prevention research (Finch, 2006). It advocates a multidisciplinary approach to sports injury prevention, including contributions from those working in epidemiology, biomechanics, sports medicine, sports science, health promotion, and behavioral psychology, as well as sports delivery and the participants themselves. Another recent framework is focused on sports safety promotion (Timpka et al., 2006) and the authors suggest that programs require that the perspective of the sports injury problem is made broader than just focusing on the individual participant. They advocate for the involvement of sports federations that are responsible for socially defined sports communities, as well as governments that represent geographically defined civic communities (Timpka et al., 2006). One of the earlier conceptual frameworks of sports injury prevention was a four-stage approach, that described the stages as being to describe the extent of the injury problem, establish the etiology and mechanisms of injuries, introduce preventive measures, and assess their effectiveness (van Mechelen et al., 1992).
Sports injury interventions have tended to focus on three main approaches: implementing education and behavior change programs, introducing regulatory/mandatory activities, and modifying the environment and equipment used (MacKay et al., 2004). Regarding injury prevention in cycling, for example, the equipment was modified through the introduction of helmets, which were designed to protect the head from injury in a collision. Educational advertising campaigns, designed to change the attitude of cyclists and increase the uptake of helmets, were delivered to the broad population as well as targeted at specific groups, such as schoolchildren. In addition, in some countries, legislation makes bicycle helmets mandatory and imposes a fine for lack of compliance. This combination of injury prevention strategies has been highly successful in countries including Australia, with a significant reduction in the rate of head injury to cyclists.
Other injury prevention strategies that are commonly adopted in sport are the use of personal protective equipment, such as helmets, faceguards, mouthguards, and padding. Taping and bracing has reduced the rate of ankle sprains in activities such as basketball. Preparticipation screening has become a commonly used method for identifying characteristics of the musculoskeletal system that may predispose an athlete to injury or for identifying incomplete recovery from a previous injury. It is then possible to identify those participants who would benefit from an intervention designed to reduce the risk of injury. More recently, studies have reported a reduction in injury rates as a result of training interventions, including strength, balance, and technique, which are usually aimed at reducing the effects of potential intrinsic risk factors. For example, balance training has been identified as a successful strategy to reduce injuries, particularly knee cruciate ligament injuries in sports such as handball. Consideration of the environment in which a sport is played has led to guidelines for many sports regarding the condition of the playing surface, for example, ensuring that the surface is even, without any potential slipping or tripping hazards. These risk management strategies are essential for the prevention of many sports injuries. Changes to rules, such as the modification of tackling rules for junior participants in football, have also been implemented. In addition, changes to sporting equipment can reduce the risk of injury; for example, the introduction of breakaway bases has significantly reduced the rate of injury in baseball and softball.
While injury prevention strategies such as these are commonplace in many sports, it is important to note that few strategies have been subject to a high-quality formal evaluation. This is particularly evident in interventions designed for young people, with many interventions designed for adults simply translated to use with children. The majority of sports injury prevention strategies appear to be based on the collective experience of people who are knowledgeable in the chosen activity. Hence, providing evidence for the effectiveness of injury prevention strategies has been identified as a priority area for continued research (Finch, 2006; MacKay et al., 2004).
Bibliography:
- Bahr R and Holme I (2003) Risk factors for sports injuries: A methodological approach. British Journal of Sports Medicine 37(5): 384–392.
- Cassell EP, Finch CF, and Stathakis VZ (2003) Epidemiology of medically treated sport and active recreation injuries in the Latrobe Valley, Victoria, Australia. British Journal of Sports Medicine 37(5): 405–409.
- Centers for Disease Control and Prevention (2002) Nonfatal sportsand recreation-related injuries treated in emergency departments: United States, July 2000–June 2001. Journal of the American Medical Association 288(16): 1977–1979.
- Conn JM, Annest JL, Bossarte RM, and Gilchrist J (2006) Non-fatal sports and recreational violent injuries among children and teenagers, United States, 2001–2003. Journal of Science & Medicine in Sport 9(6): 479–489.
- Finch C (2006) A new framework for research leading to sports injury prevention. Journal of Science & Medicine in Sport 9(1–2): 3–9.
- Finch C and Cassell E (2006) The public health impact of injury during sport and active recreation. Journal of Science & Medicine in Sport 9(6): 490–497.
- Flood L and Harrison JE (2004) Hospitalised Sports Injury, Australia 2002–03. Adelaide, Australia: Australian Institute of Health and Welfare.
- Fuller CW, Ekstrand J, Junge A, et al. (2006) Consensus statement on injury definitions and data collection procedures in studies of football (soccer) injuries. British Journal of Sports Medicine 40(3): 193–201.
- Hawkins RD and Fuller CW (1999) A prospective epidemiological study of injuries in four English professional football clubs. British Journal of Sports Medicine 33(3): 196–203.
- MacKay M, Scanlan A, Olsen L, et al. (2004) Looking for the evidence: A systematic review of prevention strategies addressing sport and recreational injury among children and youth. Journal of Science & Medicine in Sport 7(1): 58–73.
- McCrory P, Johnston K, Meeuwisse W, et al. (2005) Summary and agreement statement of the 2nd International Conference on Concussion in Sport, Prague 2004. British Journal of Sports Medicine 39(4): 196–204.
- Meeuwisse WH (1994) Assessing causation in sport injury: A multifactorial model. Clinical Journal of Sport Medicine 4: 166–170.
- Michaud PA, Renaud A, and Narring F (2001) Sports activities related to injuries? A survey among 9–19 year olds in Switzerland. Injury Prevention 7(1): 41–45.
- Orchard J, Newman D, Stretch R, Frost W, Mansingh A, and Leipus A (2005) Methods for injury surveillance in international cricket. Journal of Science & Medicine in Sport 8(1): 1–14.
- Potter Forbes M and Aisbett C (2003) Injury Costs! A Valuation of the Burden of Injury in New South Wales 1998–1999. Sydney, Australia: NSW Injury Risk Management Research Centre.
- Schneider S, Seither B, Tonges S, Schmitt H, and Zimmermann-Stenzel M (2006) Sports injuries: Population based representative data on incidence, diagnosis, sequelae, and high risk groups. British Journal of Sports Medicine 40(4): 334–339.
- Timpka T, Ekstrand J, and Svanstrom L (2006) From sports injury prevention to safety promotion in sports. Sports Medicine 36(9): 733–745.
- van Mechelen W, Hlobil H, and Kemper HC (1992) Incidence, severity, aetiology and prevention of sports injuries: A review of concepts. Sports Medicine 14(2): 82–99.
- Watson WI and Ozanne-Smith J (1998) The Cost of Injury to Victoria. Melbourne, Australia: Monash University Accident Research Centre.
- Bird S, Black N, and Newton P (1997) Sports Injuries: Causes, Diagnosis, Treatment and Prevention. Cheltenham, UK: Stanley Thornes.
- Caine DJ, Caine CG, and Lindner KJ (eds.) (1996) Epidemiology of Sports Injuries. Champaign, IL: Human Kinetics.
- Caine DJ and Mafulli N (eds.) (2005) Special Issue: Epidemiology of Pediatric Sports Injuries: Individual Sports. Medicine and Sport Science 48: .
- Mafulli N and Caine DJ (eds.) (2005) Special Issue: Epidemiology of Pediatric Sports Injuries: Team Sports. Medicine and Sport Science 49: .
- McClure R, Stevenson M, and McEvoy S (eds.) (2004) The Scientific Basis of Injury Prevention and Control. Melbourne, Australia: IP Communications.
- Peterson L and Renstro¨ m P (2001) Sports Injuries: Their Prevention and Treatment, 3rd edn. London: Martin Dunitz.
- Renstro¨ m PAFH (ed.) (1993) Encyclopaedia of Sports Medicine, Vol IV: Sports Injuries: Basic Principles of Prevention and Care. Oxford, UK: Blackwell Scientific Publications.
- http://www.acc.co.nz – Accident Compensation Corporation.
- http://www.sportsmed.org – American Orthopaedic Society for Sports Medicine.
- http://www.injuryupdate.com.au – Injuryupdate.com.
- http://www.nlm.nih.gov/medlineplus/sportsinjuries.html – MedlinePlus Sports Injuries.
- http://www.smartplay.com.au – Smartplay.
- http://www.sma.org.au – Sports Medicine Australia.
- http://www.sportsinjuryclinic.net – Virtual Sports Injury Clinic.
See also:
Free research papers are not written to satisfy your specific instructions. You can use our professional writing services to buy a custom research paper on any topic and get your high quality paper at affordable price.
ORDER HIGH QUALITY CUSTOM PAPER

Always on-time

Plagiarism-Free

100% Confidentiality



