
This sample Occupational Death and Injury Rates Research Paper is published for educational and informational purposes only. If you need help writing your assignment, please use our research paper writing service and buy a paper on any topic at affordable price. Also check our tips on how to write a research paper, see the lists of health research paper topics, and browse research paper examples.
Introduction
Work-related injury and disease, whether fatal or nonfatal, is an important cause of morbidity and mortality in all countries of the world. Most aspects of society are affected, as the injury or illness impacts not just on the injured or sick person, but also on their family, friends, and workmates. Tragically, most work-related deaths (and nonfatal conditions) are preventable and therefore should not occur, but this preventability has a positive aspect, because it means that there is an opportunity to decrease the current burden from work-related injury and illness. Understanding the scope of the problem, and how and why work-related fatal and nonfatal disorders occur, is an important first step in their prevention. This research paper aims to support this understanding by providing an overview of work-related injury and illness, focusing on fatal conditions, but including serious nonfatal conditions also. The scope covers the burden of work-related ill health in societies around the world, as well as information on the type of disorder and, particularly for injury, the circumstances in which the disorders occur.
Definitions
When considering work-related injury or illness, it is important to have a clear definition of ‘work-relatedness.’ This concept is not always straightforward and has been applied differently in different settings and by different authors. A reasonable general definition of work-relatedness is that the disorder results from a work exposure. That is, work-related exposures must have contributed as a necessary factor to the individual injury or illness.
Usually, it is clear whether or not someone is employed, but this may not be the case when the arrangements are less formal, such as family members helping out in a family business (e.g., a shop or a farm), or ad hoc work such as collecting discarded cans for recycling. These more informal arrangements occur in all societies, but are particularly common in developing countries. In the case of disease, the condition may well not become manifest until the affected person has changed jobs or retired, making the connection to work difficult to recognize or establish. Work-related disorders may even affect persons who are not employed at the time of injury or the relevant exposure. This is because persons who are not working (bystanders) can be harmed as a result of the work activity of others (e.g., a visitor to a factory being hit by a forklift truck, or a community living around a smelter affected by contaminated runof f ).
The context of the work activity is often of importance in terms of prevention and is also commonly used as the basis for inclusion or exclusion of cases. This is particularly so for work-related injury of working persons, which can be usefully divided into three groups – injuries that occur in traffic incidents on public roads in the course of work (‘work-road injuries’); other injuries that occur in the course of work (‘workplace injuries’); and injuries that occur while traveling to or from work (‘commuting injuries’). Workplace and work-road injuries are commonly combined into a single measure of work-related injuries of workers (‘working injuries’). Most injury studies include working injuries. Commuting injuries are included less consistently.
Global Burden Of Occupational Injury And Disease
Fatal Injury
Occupational injury is an important cause of mortality and morbidity throughout the world, in both developing and developed countries. The extent of the burden arising from occupational injury is difficult to determine accurately, and what information is available primarily arises from specific studies designed to assess the burden. This is true at a national and international level. Developing accurate estimates is even more difficult at an international level, but in recent years several attempts have been made. The estimates of the annual number of injury deaths of workers vary from about 140 000 to nearly 500 000, with a best estimate of about 350 000. This includes workplace and work-road deaths, but largely excludes commuting deaths, for which there are no soundly based estimates. The main problems with the global estimates are a widespread lack of data, the ‘contamination’ of injury data by the inclusion of some disease cases in some countries, and the inconsistent inclusion of homicides, suicides, and commuting deaths (Driscoll et al., 2005c).
There are no global or regional estimates of bystander injury deaths, but bystander death is an important occupational injury issue, and some idea of the scope of the problem is given by two national studies. These studies found that the number of workplace bystander deaths was between one-tenth (New Zealand) and one-quarter (Australia) of the number of workplace deaths. In Australia the number of road bystander deaths (nonworking persons killed in motor vehicle incidents on public roads in which the working vehicle was ‘at fault’) was similar to the number of work-road deaths.
Fatal Disease
As with injury, occupational disease is an important cause of mortality and morbidity throughout the world, but the extent of the burden is much more difficult to quantify. This is because most diseases can have a number of possible causative exposures or exposure circumstances and take many years to become fully developed, which makes it extremely difficult to establish a connection between work exposures and a resulting disease in an individual case. This has meant that epidemiological approaches, particularly population attributable risk (PAR) techniques, have been used. These require an estimate of the risk arising from exposure, and of the prevalence of exposure. Risk information is obtained from epidemiological studies and is probably broadly generalizable from one exposure circumstance to another. Reliable exposure information is commonly not available, or inconsistently available, for many countries. This has meant that extrapolation between countries and time periods is commonly required for national and global estimates.
As for injuries, several attempts have been made in recent years to establish global estimates of occupational disease. The estimates of the annual number of disease deaths of workers vary from about 325 000 to about 1.6 million, with the higher estimates probably the most accurate (Driscoll et al., 2005c). The recent Comparative Risk Assessment project of the World Health Organization (WHO) provided global estimates of fatal (and nonfatal) disease arising from carcinogens (Driscoll et al., 2005a), airborne exposures (Driscoll et al., 2005b), and injury risk factors (Concha-Barrientos et al., 2004). The disease estimates from the various studies have considerable uncertainty, arising in particular from missing, sparse, or old information on exposure and overall rates of death for specific diseases, and varying inclusion and exclusion criteria. There are no estimates at either national or global level of bystander disease deaths.
Nonfatal Injury And Disease
Global estimates of injury and disease usually focus on mortality, mainly because in the statistics collected by countries and institutions the mortality data are generally more comprehensive. However, nonfatal conditions can still result in considerable morbidity. Because it can be difficult to compare or combine the burdens arising from fatal and nonfatal conditions, several measures have been developed to enable this to be done. The most commonly used such measure is the disability-adjusted life year (DALY), which is a weighted estimate of the number of years lived with disability. The severity of the disability is described by the weighting. The DALY therefore represents the gap between the current situation and an ideal situation in which everyone achieves an agreed standard life expectancy in perfect health (Driscoll et al., 2005a).
On the basis of DALYs, which allow both fatal and nonfatal disorders to be included, the recently completed Comparative Risk Assessment project estimated that work-related exposures were responsible at a global level for about 37% of back pain, 16% of hearing loss, 13% of chronic obstructive pulmonary disease, 11% of asthma, 9% of lung cancer, 8% of injuries, and 2% of leukemia. Looking only at health-care workers, about 40% of hepatitis B and hepatitis C infections and 4.4% of HIV infections in these workers were estimated to be due to needlesticks (Concha-Barrientos et al., 2004).
Work-Related Injury And Disease Deaths In Various Countries
Injury
Work-related fatal injury is a high-profile issue in many countries, both developed and developing. Overall estimates from studies have been produced for various countries, including Australia, Denmark, Finland, Jordan, New Zealand, and the United States. Most of these studies counted the number of injury deaths using coroners’ data and/or death certificates. All of the studies included workplace deaths, most included work-road deaths, and some included commuting deaths. Countries and regions for which one or more detailed study or review articles addressing work-related fatal injuries have been published include Australia, Brazil, Canada, China, Denmark, Europe, Finland, Iceland, Italy, Jordan, Kuwait, New Zealand, Nigeria, Scandinavia, South Africa, Sweden, Taiwan, the United Kingdom, and the United States. Comparisons between studies or countries of rates and types of fatal work-related injuries have many potential pitfalls. These arise because of differences in the definitions of work relatedness, and differences in the inclusion and exclusion criteria, which may be based on age, sex, occupation, industry, employment arrangement, or incident type. Even when the definitions and criteria are apparently similar, appropriate comparisons should be undertaken on a limited, well-defined basis, such as using industry, occupation, and/or age, or using overall results adjusted for differences in these potential confounders. A recent example of a comparison that attempted to take account of the factors compared fatalities in New Zealand, Australia, and the United States. In this study, the raw fatality rates per 100 000 persons per year were 4.9 (New Zealand), 3.8 (Australia), and 3.2 (United States). Most of the differences were found to be due to differences in industry distribution. Once this was taken into account, the Australian and U.S. rates were found to be very similar, and the New Zealand rate was found to be only 10 to 15% higher (Feyer et al., 2001). Other studies have compared New Zealand with other countries, the United States with Australia, Great Britain with Europe and the United States, or have compared results between countries as part of analyses that focused on specific industries, occupations, or factors.
Disease
National estimates of work-related disease deaths have been produced for Australia, Canada, Finland, New Zealand, and the United States. All these studies relied on the PAR approach to produce their estimates. Direct comparison between countries is not common and has the same problems as comparisons on the basis of injury, with these problems usually more important and harder to overcome when studying disease.
Common Characteristics Of Work-Related Fatal Injuries And Diseases
The ultimate aim of the study of work-related injuries and diseases is to prevent their occurrence. General surveillance and maintenance of national statistics makes an important contribution to this by providing an understanding of the frequency and rate of such deaths, changes in these parameters over time, and differences between different regions, industries, occupations, or countries. All of these may provide evidence of approaches to prevention that are apparently successful or not successful, or identify hazards and associated risks that need to be controlled. However, the design of appropriate interventions requires a thorough understanding of the circumstances surrounding fatal incidents, looking for common patterns that might be amenable to preventative interventions. Such an understanding usually only comes from a detailed study of a well-circumscribed area, focusing on factors such as a particular industry, occupation, mechanism, agency, exposure, or personal characteristic. There have been many examples of studies that have focused on such areas. This section summarizes the main approaches that have been taken.
Injuries
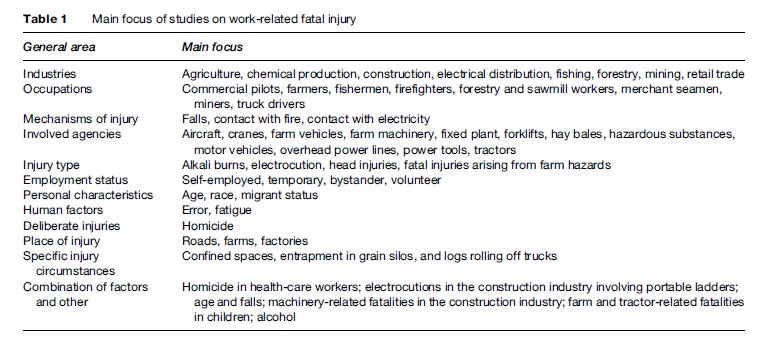
Published studies of work-related fatal injuries may include all work-related injury deaths or may focus on particular regions, industries, occupations, mechanisms, involved agencies, injury type, personal characteristics, human factors, intent, place of injury, and specific injury circumstance (see Table 1 for selected examples). Some of the important findings arising from these studies are considered here.
Age And Gender
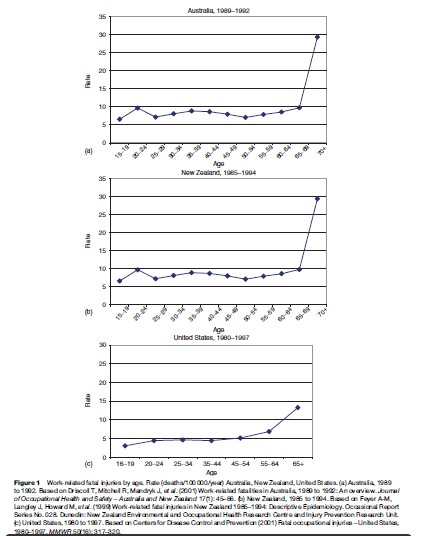
Most studies have found a much higher rate of work-related fatal injury in men than in women. However, this is probably mainly a result of differences in the type of job (the occupation, specific task, and industry) performed by them. Similarly, most studies have found that the rate of work-related fatal injury is fairly constant until about the age of 60 or 65, after which time the rate of injury increases dramatically (see Figure 1). There are a number of plausible explanations for this finding, including older people being more likely to be injured or to die from a given injury than younger workers. However, it may also be partially artifactual, resulting from undercounting in the number of people at risk (i.e., older working people may not have been properly recorded as part of the labor force). This is especially an issue for elderly farmers, who may continue to work but not be recorded as workers in population surveys, thereby producing an erroneously low denominator and a correspondingly erroneously high fatality rate. There is also a worrying number of deaths of young workers associated with farm work.
Industry And Occupation
Certain occupations and industries have been consistently found to have a high rate of work-related fatal injury (see Table 1). The occupations include commercial pilots, loggers, fisherpersons, miners, truck drivers, and farmers. High rates are commonly seen in the forestry and logging, fishing, mining, agriculture, transport, and construction industries. These high rates presumably reflect high risks of exposure to serious hazards. It is usually more valuable to examine occupation (what people do) rather than industry (where people work), because the risks are usually similar in the same occupation regardless of industry (e.g., truck drivers in the agriculture, manufacturing, mining, and transport industries probably face similar hazards and associated risks). In contrast, a single industry usually comprises a range of occupations with very different risks (e.g., an office worker, an electrician, a driver, and a painter all employed in the same construction company would generally face different hazards). Within each area it is helpful to use as narrowly defined subgroups as the data will allow. For example, the high rates for forestry, mining, and structural steel laborers and fishermen/ women are hidden by the overall rate for the relevant larger occupation group to which they usually belong (‘Laborers and related workers,’ or something akin to this).
Mechanism
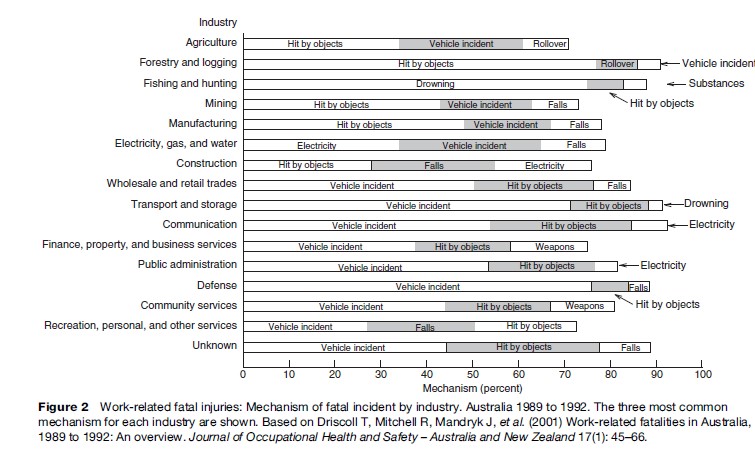
Vehicular incidents on public roads are often found to be the most common single mechanism of fatal incident for most occupation groups and many industry groups. Falling from a height, falling objects hitting persons, and contact with electricity are other common mechanisms seen across a number of different occupation and industry groups (see Figure 2).
Place
Work-related fatal injuries in persons from particular occupations or industries occur in many different places, so a single place such as a farm or a mine is not a very sensitive indicator of fatalities in specific occupations or industries such as farming or mining. However, some places are likely to have a high specificity for work-related fatal injuries. For example, the vast majority of nonsuicide fatal injuries occurring in mines or on farms are likely to be related to work or work-related exposures, but many injuries occurring to farmers do not occur on farms, and many injuries to miners do not occur on mine sites. Motor vehicle incidents are usually the most common single mechanism resulting in the fatal injury of working persons, and it is not surprising that the most common place for these fatal incidents is public roads of some sort. However, many vehicle incidents also occur in other workplaces, such as farms, trade areas, and mines.
Cause Of Death
The cause of death is likely to vary with the circumstances of the incident. So, although knowledge of the cause of death is helpful when identifying opportunities for, and approaches to, prevention, such information is best combined with other relevant information. For example, in a study of work-related fatal injury in Australia, mechanical asphyxia accounted for 7.4% of all deaths and 7.9% of workplace deaths. However, it was the cause of death in 45% of deaths involving persons being trapped by machinery, 25% of deaths involving the rollover of mobile mechanical equipment, and 17% of deaths involving persons being hit by falling objects (Driscoll et al., 2001). This type of information is important because such incidents are potentially survivable if the person has not sustained severe injuries. In many of these incidents, the worker was working alone, and it is possible that the worker may not have died if there was someone else nearby at the time of the incident who could have freed the injured worker. This has implications for the working procedures used in particular situations (e.g., whether persons are allowed to work alone) and in assessing the possible usefulness of systems for contacting someone in the event of an emergency.
Alcohol And Drugs
The role of alcohol and drugs in work-related fatal injury is controversial. Most studies have found that alcohol and drugs contribute in a meaningful way to about 5% of the deaths of workers. Alcohol is probably a larger problem than drugs, but the relative contribution is likely to vary between working circumstances. For example, stimulant use is likely to be more widespread, and more likely to contribute to injury occurrence, in truck drivers than in many other occupations. Since alcohol and drug use in connection with work is potentially preventable through appropriate education and other programs, alcohol and drug use should be considered in occupational health and safety (OHS) prevention programs.
Time Of Day
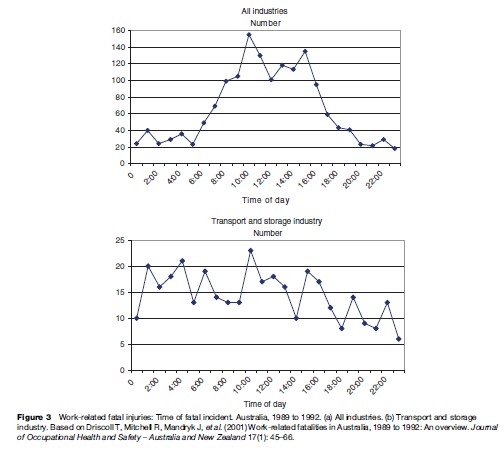
Most studies that have examined the time of day of fatal incidents have found mid-morning and mid-afternoon peaks. This has been seen across many industries (e.g., fishing, forestry, and mining) and reported by a number of studies. It is likely that the main reason for this pattern is that these are the times when the largest number of people are working, implying that the risk to the individual worker is no higher than at other times (unfortunately, appropriate denominator data are rarely available, meaning that rates can’t be calculated). An alternative explanation, which might make some contribution, is that the peak times may be when the activities are more complicated or interact more, when people are becoming fatigued several hours after the last break or meal, when people are anticipating a break, or some combination of these or other factors. For other industries, such as the transport industry, the time of the fatal incident is usually more evenly spread across 24 hours, presumably reflecting the fact that the transport industry functions at a high level at most hours (see Figure 3). However, it should also be kept in mind that fatigue appears to be an important problem in long-distance truck drivers, and so higher relative frequencies of incidents occurring overnight might reflect a much greater risk for drivers during these early morning hours, with fatigue and darkness plausible explanations for this.
Diseases
As for injury, published studies of work-related fatal disease may include all work-related disease deaths or focus on particular diseases such as cancer, heart disease, infectious disease, neurological disease, and so on. Studies have also focused on particular regions, industries, occupations, and exposures.

Disease Types
On a global basis, malignant neoplasms, communicable diseases, circulatory diseases, and respiratory diseases are the main causes of work-related fatal disease (Driscoll et al., 2005a; Hamalainen et al., 2007). In the WHO Comparative Risk Assessment project (which could not include a consideration of communicable diseases and some other diseases because the global data were inadequate to allow the Comparative Risk Assessment methodology to be applied), the main causes of disease mortality were found to be chronic obstructive pulmonary disease (59% of occupational disease deaths), lung cancer (19%), mesothelioma (8%), asthma (7%), coal workers’ pneumoconiosis (3%), silicosis (2%), asbestosis (1%), and leukemia (1%) (Concha-Barrientos et al., 2004).
Age And Gender
Fatal occupational disease is nearly exclusively a problem of older and retired workers, apart from deaths from communicable disease. This is because the conditions likely to prove fatal usually have a long period between exposure and when the condition becomes evident. As with injury, rates of most types of work-related fatal disease are much higher in men than in women, and this almost certainly reflects the type and level of their respective exposures at work. One exception to this is communicable diseases, which are estimated to be much more common in women than men as a cause of work-related mortality, especially in developing countries where women work in occupations with a high risk of exposure to infective agents (Hamalainen et al., 2007).
Industry And Occupation
Certain occupations and industries have associated harmful exposures that significantly increase the risk of developing a condition that leads to premature death. High-risk exposures that have been a major problem in the recent past include asbestos (in mining, manufacturing, and construction), silica (mining and construction), benzene (manufacturing), chlorinated organic solvents (manufacturing), and pesticides (farming). Most of the more obvious causative exposures that typically caused cancer or severe lung disease are now well-controlled in the majority of workplaces in developed countries, but control is still poor in many developing countries and is not always optimal in developed countries. In addition, less obvious issues have been recognized, such as the balance between job demands and job control, that have been found to be associated with the development of ischemic heart disease and, because ischemic heart disease is so common, to result in a considerable number of work-related deaths.
Nonfatal Injury And Disease
Injury
The Connection Between Fatal And Nonfatal Injury
The circumstances surrounding fatal work-related incidents are probably representative of the circumstances surrounding many major nonfatal injuries and probably many minor injuries and near misses, but appear not to be representative of all injuries. For example, certain nonfatal injury types such as injuries of the back from sprain/ strain, overuse injuries of the limbs, and simple cuts from hand tools rarely cause death. However, for many other injury circumstances, it is probably just a matter of chance as to whether the affected person is killed, injured, or just involved in a near miss. Common examples of this include most electrocutions, falls, and drowning, as well as most injuries resulting from motor vehicle incidents or the use of fixed or mobile mechanical equipment. In addition, for the vast majority of nonfatal injuries, there is little or no useful information recorded by the workplace, and even fewer nonfatal injuries are investigated by OHS jurisdictions and/or the police. Even where incidents are investigated, the data are usually not available in a form that facilitates systematic study. Therefore, more is known about fatal injury, and the study of fatal injury also provides information on factors that are relevant to many nonfatal injuries.
Lost time injury measures (which count injuries that result in one or more days off work) are commonly used to monitor levels of OHS. However, the measures are open to manipulation and subject to deliberate or unintentional variations in reporting efficiency, making interpretation and comparisons more difficult. In contrast, deaths are hard to cover up or ‘lose.’ Also, although both fatal and lost time injury end points can have some definitional problems, with death these problems are on the margins, whereas with nonfatal injury the definitional problems can be of major importance.
One consistent difference is in the relationship to age, with the rate of nonfatal injuries being highest in young workers. Much of this difference is probably due to the varying risks faced by workers of different ages, but higher rates have still been found even when differences in job characteristics are taken into account.
The study of nonfatal injury and fatal injury should be seen as complementary. For year-to-year measures within a company or small industry group, nonfatal injury (or some form of process measure) is the appropriate outcome to use. Whether this outcome is defined further as the lost time injury rate, or in some other form, is less of an issue. However, for national or international comparisons, for industry comparisons, for occupational comparisons, and for identification of common circumstances or patterns associated with incidents that result in injury, information on work-related fatal injury, usually obtained from some form of coroner’s system, is the most reliable form of data to use to monitor general levels of OHS related to most forms of injury.
Common Characteristics Of Work-Related Nonfatal Injuries
Studies of nonfatal work-related injury have a similar focus to studies of fatal injury, except that there are few studies at the international or even national level. As mentioned, many serious nonfatal injuries are similar in nature, character, and circumstance to fatal injuries, but there are also some types of injuries that are rarely or virtually never fatal. In addition, the identified characteristics of work-related nonfatal injury depend considerably on the working group being studied and the data source being used (e.g., workers’ compensation data, hospital emergency department data, hospital admissions data, or data from a specific cohort of workers). Key aspects of nonfatal injuries that differ from fatal injuries are that the common injury types across most industries are laceration, fracture, or sprain/strain of the hands (including the fingers) and injuries to the eye, most commonly by foreign bodies. In some industries and occupations, sprain/strain of the back is also common. Common characteristics of the circumstances associated with these injuries are using powered or non-powered tools (hand and eye injuries) and manual handling of heavy objects or working with repetitive or awkward postures.
Disease
The Connection Between Fatal And Nonfatal Disease
Many of the causative exposures and exposure circumstances leading to fatal disease can also lead to nonfatal disease, either resulting in the same condition or related conditions. For example, exposure to asbestos can lead to malignant mesothelioma, which is nearly always fairly rapidly fatal; lung cancer, which is often fatal but not always so; and asbestosis, a fibrotic disease of the lung that can be fatal but more commonly isn’t, although it can result in severe disability due to respiratory disease. Exposure to ultraviolet radiation can lead to malignancies of the skin, which are more commonly not fatal than fatal. There are a wide variety of occupational exposures that can cause or exacerbate the symptoms of asthma, the severity of which can vary between mild, debilitating, or even fatal. Dermatitis due to work exposures can be mild or very debilitating but is very rarely fatal. Much disease related to work, whether fatal or nonfatal, is hard to identify as being work-related because of the long latency between exposure and disease diagnosis, and because most diseases can be caused by more than one exposure. The available records usually provide better coverage of disease deaths than nonfatal disease cases, especially in developing countries, but for most disease types the connection to work is difficult to establish regardless of the severity of disease. Therefore, study of fatal disease deaths also provides information on factors that are relevant to many nonfatal diseases, but study of nonfatal disease is still necessary because some diseases rarely, if ever, lead to death and the connection to work is hard to identify for disease deaths. As for injuries, the characteristics of work-related nonfatal disease depend considerably on the working group being studied and the data source being used. Respiratory disease, ischemic heart disease, musculoskeletal disease, noise-induced hearing loss, and dermatitis are key nonfatal diseases, with the latter three in particular not a feature of fatal work-related disease. As indicated by the global estimates, these diseases result in a huge burden of work-related ill health.
Approaches To Studying And Obtaining Information On Work-Related Injury And/Or Disease
Most of the studies of work-related fatal injury are essentially cohort studies of the population of interest, with the population being all working persons or subgroups of the population identified by characteristics such as occupation, industry, age, or sex. However, other approaches have been used (e.g., case-control studies, capture-recapture studies, and proportional mortality studies) or could be used (e.g., case-crossover design). Sometimes the analysis focuses on frequencies and percentages, but usually rates are presented, at least at an overall level. Comparisons are made on the basis of frequency, percent, and/or rate, with the effect of multiple exposures of interest controlled by stratification or exclusion. Other approaches have included Poisson regression or other regression methods, the use of standardized or proportional mortality ratios, and the calculation of lifetime risk or years of life lost.
Disease studies commonly focus on individual worker groups. Cohort approaches are often used, but case-control designs, and to a lesser extent cross-sectional designs, are more commonly used than they are for injury studies. The main outcomes of interest are relative risks (or odds ratios), standardized mortality ratios, proportional mortality ratios, and DALYs, which have become a commonly used measure in some settings. As mentioned earlier, studies assessing burden commonly make use of the population attributable risk approach. More detail on these approaches is available in many good epidemiology references (Rothman and Greenland, 1998; Checkoway et al., 2003).
Data Sources For Identifying Work-Related Injuries And Disease
In most developed countries and some developing countries, routine data systems probably provide reasonable coverage of severe and fatal injuries for the employees and industry sectors that they do cover (although some underenumeration can be expected, even for deaths). Disease deaths and serious disease cases may also be recorded, although the routine systems rarely identify the work-relatedness of an individual case. Cases recorded by available data systems and reported to the WHO or the International Labor Organization have been used as the basis for estimating the global number of work-related injury (and disease) cases. The main examples of useful data sources are summarized here.
Death Certificates
Since a death certificate should be completed for all deaths, death certificates form a potential source of information on work-related injury and disease deaths if information on the certificate is able to be used to identify such deaths. This information is usually only of direct use for injuries, unless the disease is of a sort that is explicitly connected to work (such as coal workers’ pneumoconiosis or silicosis). For injury, if work-relatedness is explicitly coded, it is usually identified by a box that can be checked if the death is related to work or occurs at work. The U.S. National Traumatic Occupational Fatalities surveillance system, which is run by the National Institute for Occupational Safety and Health, is the best example of the use of death certificate information for surveillance purposes. Some information is coded, but most of the available information is in narrative form. Although this has disadvantages, narrative information is very useful because it allows searches to be conducted on a wide variety of particular topics.
Death certificates provide a relatively low-resource approach to work-related fatal injury surveillance. Coverage of work-related deaths should not be influenced by employment arrangement, job type, or marital status, factors that by design or practice can exclude deaths from being included in compensation systems. However, there are limitations to the usefulness of death certificates for injury. These include incomplete coverage, inconsistent information on certificates because of the many different people involved in completing them, lack of uniform coding of information provided on the certificate, lack of relevant information on occupation and industry of the person, and lack of detailed information.
Workers’ Compensation Information
Information systems based on compensation claims usually have the advantage of reasonably up-to-date and independently verified information, but the disadvantage of deliberate limitations in the coverage of some workers and the practical exclusion of some others. Examples include the Berufsgenossenschaften in Germany, provincial-based systems in Canada, and the National Data-Set for Compensation-Based Statistics in Australia. All these systems provide information on both injury and disease, although injuries are generally better covered. For each of these systems, and for other compensation systems, there are concerns that the coverage is incomplete and that the extent of this incompleteness is uncertain, although it is of the order of 40% in Australia for work-related fatal injury and probably is similar elsewhere (Driscoll et al., 2003).
OHS Authority Reports
Most countries have one or more state or federal government occupational health and safety authorities that investigate some work-related incidents and keep statistics regarding them. These are a potentially very useful source of information on work-related injury, since they often contain detailed information. However, the information provided by these agencies can have many shortcomings, being influenced by changes in administrative policy, varying approaches to coding, and variable coverage.
A good example of work-related fatality surveillance using information from official statistics held by OHS authorities is the Reporting of Injuries, Disease and Dangerous Occurrences Regulations (RIDDOR) system. The RIDDOR data are used as the basis of information published by the Health and Safety Executive (HSE) in the United Kingdom. RIDDOR is based on notifications to the HSE required by statute. Like most systems that rely on notifications to OHS authorities, or investigation by the OHS authorities, work-related deaths that are covered by other agencies for the purposes of reporting or investigation are not included within RIDDOR statistics. These include deaths related to the supply or use of flammable gas, most deaths related to marine fishing and merchant shipping, fatal injury associated with civil aircraft flight or with premises covered by the relevant explosives act, and deaths arising from motor vehicle crashes on public roads. Therefore, again like most systems based on OHS notifications and inspections, the RIDDOR system covers the majority of work-related injury deaths of workers, while probably missing a substantial minority of those deaths. Some information on bystander deaths is included, but coverage is probably poor.
Coroners’ Data
The advantages and disadvantages of using coroners’ data as a source of information on work-related injury deaths have already been mentioned. In brief, all injury deaths, including those that are related to work, are due to some form of external cause, and so can be expected to be reported to the coroner (as required by law in most developed countries). All deaths reported to the coroner are the subject of some form of investigation, and the information collected during a coroner’s investigation is often very detailed and can contain useful information for descriptive and preventive purposes. The size and completeness of the data set allows patterns of circumstances to be seen that would not be noticed when a more limited group of incidents was examined; and the information contained in coroners’ files is theoretically available to persons with bona fide reasons for accessing it. Problems with using the coroners’ system (or medical examiner system in some places in the United States and Canada) as a source of information include a lack of standardized classification and investigation approaches, lack of mutually exclusive classification categories, incomplete coverage, lack of relevant information in the coronial files, lack of a centralized file storage system, and reliance on paper records. Some countries are moving to overcome these difficulties by developing a computerized database of all deaths reported to the coroner, although Australia is probably the only country where such a system is fully functional (Monash University National Centre for
Coronial Information (MUNCCI), 2001). The coroners’ system is not a good source of information on work-related disease deaths because, with some minor exceptions, these do not fall under the area of interest of the coroners’ system. Coroners’ records have been most comprehensively used as a source of information on work-related fatal injuries in Australia and New Zealand.
Hospital Admissions
Many countries have begun collecting information on the type and cause of hospital admissions. Some of these systems use codes that identify a connection to work. This is primarily of use for (nonfatal) work-related injury cases, because the connection between work and disease is often not recognized.
Emergency Department Presentations
Emergency department data systems are also increasingly being used as sources of information on various types of injury, including work-related injury, in persons that present to emergency departments. Like the hospital data, the emergency department systems appear to be of little use as a source of information on work-related disease.
Multiple Sources
Some fatal injury data systems attempt to use information from multiple sources. Probably the best of these is the Census of Fatal Occupational Injuries (CFOI), which is run by the U.S. Bureau of Labor and Industry and was introduced in 1992. This system uses death certificate information, but complements it with information from workers’ compensation reports, coroners, the Occupational Safety and Health Administration, police, and the media. A unique aspect of the CFOI system is that some follow-up of surviving persons is undertaken. There is no equivalent system collecting information on work-related disease.
Company Data
Data maintained by companies in personnel and job assignment records are often used in studies to assess the relationship of exposure to a particular disease outcome. Exposure measures can be based on the duration of exposure, the level of exposure, or some combination of the two. Large-size cohort studies can be based on collection, and a common analysis, of data from several companies making the same products. The International Agency for Research on Cancer has broadened these analyses to a global level for a number of work-related (and other) exposures, such as sulfuric acid mist, wood dust, manmade mineral fibers, and formaldehyde.
Surveys
Many countries conduct national or regional surveys that include questions on occupational injuries and illnesses. For example, the U.S. Bureau of Labor Statistics conducts annual surveys of occupational injuries and illnesses, and the Australian Bureau of Statistics conducts national health surveys approximately every five years. Such surveys are usually based on self-report.
The Press
Several studies have used press clippings and radio reports as a source of information on work-related fatal injury, but usually as an adjunct to other information sources rather than as the primary data source. Some information on work-related disease is available from the press, but this is ad hoc and not amenable to use for surveillance or other purposes.
Conclusion
Work-related injury and disease is a significant cause of injury and disease at national and global levels. It is important to obtain reliable information on the burden arising from work, and the exposures leading to this burden, in order to prioritize and plan appropriate interventions. Such interventions are considered in various general texts (e.g., see Agius and Seaton, 2005).
Bibliography:
- Agius R and Seaton A (2005) Practical Occupational Medicine. London: Hodder Arnold.
- Checkoway H, Pearce N, and Kriebel D (2003) Research Methods in Occupational Epidemiology. New York: Oxford University Press.
- Concha-Barrientos M, Nelson D, Driscoll T, et al. (2004) Selected occupational risk factors. In: Ezzati M, Lopez A, Rodgers A and Murray C (eds.) Comparative Quantification of Health Risks: Global and Regional Burden of Disease Attributable to Selected Major Risk Factors, vol. 2, pp. 1651–1802. Geneva, Switzerland: World Health Organization.
- Driscoll T, Mitchell R, Mandryk J, et al. (2001) Work-related fatalities in Australia, 1989 to 1992: An overview. Journal of Occupational Health and Safety – Australia and New Zealand 17(1): 45–66.
- Driscoll T, Mitchell R, Mandryk J, et al. (2003) Coverage of work-related fatalities in Australia by compensation and occupational health and safety agencies. Occupational and Environmental Medicine 60: 195–200.
- Driscoll T, Nelson D, Steenland K, et al. (2005a) The global burden of disease due to occupational carcinogens. American Journal of Industrial Medicine 48: 419–431.
- Driscoll T, Nelson D, Steenland K, et al. (2005b) The global burden of non-malignant respiratory disease due to occupational airborne exposures. American Journal of Industrial Medicine 48: 432–445.
- Driscoll T, Takala J, Nelson D, et al. (2005c) Review of estimates of the global burden of injury and illness due to occupational exposures. American Journal of Industrial Medicine 48: 491–502.
- Feyer A-M, Williamson A, Stout N, et al. (2001) Comparison of work-related fatal injuries in the United States, Australia, and New Zealand: Method and overall findings. Injury Prevention 7(1): 22–28.
- Hamalainen P, Takala J, and Saarela K (2007) Global estimates of fatal work-related diseases. American Journal of Industrial Medicine 50(1): 28–41.
- Monash University National Centre for Coronial Information (MUNCCI) (2001) Data Dictionary for the National Coroners Information System, version 1. Melbourne, Australia: Monash University.
- Rothman K and Greenland S (1998) Modern Epidemiology. Philadelphia, PA: Lippincott Williams and Wilkins.
- Feyer A-M and Williamson A (eds.) (1998) Occupational Injury: Risk, Prevention and Intervention. London: Taylor and Francis.
- Fingerhut M, Nelson DI, Driscoll T, et al. (2006) The contribution of occupational risks to the global burden of disease: Summary and next steps. La Medicina del Lavoro 97(2): 313–323.
- Nelson DI, Concha-Barrientos M, Driscoll T, et al. (2005) The global burden of selected occupational diseases and injury risks: Methodology and summary. American Journal of Industrial Medicine 48: 400–418.
- Nurminen M and Karjalainen A (2001) Epidemiologic estimate of the proportion of fatalities related to occupational factors in Finland. Scandinavian Journal of Work, Environment and Health 27: 161–213.
- Steenland K, Burnett C, Lalich N, et al. (2003) Dying for work: The magnitude of U.S. mortality from selected causes of death associated with occupation. American Journal of Industrial Medicine 43: 461–482.
See also:
Free research papers are not written to satisfy your specific instructions. You can use our professional writing services to buy a custom research paper on any topic and get your high quality paper at affordable price.
ORDER HIGH QUALITY CUSTOM PAPER

Always on-time

Plagiarism-Free

100% Confidentiality


