
This sample Physical Activity and Health Research Paper is published for educational and informational purposes only. If you need help writing your assignment, please use our research paper writing service and buy a paper on any topic at affordable price. Also check our tips on how to write a research paper, see the lists of health research paper topics, and browse research paper examples.
Introduction
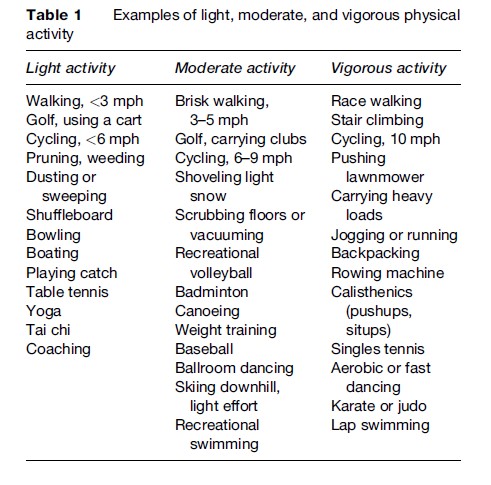
Physical activity can be defined as any movement that substantially increases the amount of calories that an individual burns in a day. Walking, gardening, washing the car, dancing, raking, swimming, and jogging are all types of physical activity. However, as most people know, not all activities burn the same amount of calories. Activities that require modest energy expenditure and, therefore, burn fewer calories per hour are considered light or moderate, while those that burn more calories per hour are considered vigorous or strenuous. Examples of each type are included in Table 1. Individuals can burn the same amount of calories by engaging in moderate activity for an extended period of time as they can by engaging in vigorous activity for a shorter period of time. What has remained questionable, however, is whether moderate activity and vigorous activity confer the same health benefits in terms of chronic disease risk, mental health, and mortality.
In this research paper, we consider beneficial effects of physical activity on health. The paper begins by reviewing the evidence that regular physical activity reduces the risk of a number of specific disease conditions. It considers methodologic considerations that have been addressed in determining the relationships between physical activity and these conditions are causal. This research paper discusses guidelines proposed by various organizations regarding the optimal level of physical activity for overall health. It considers clinical and public health strategies that can be used to increase physical activity in the population, and concludes with a discussion of safety considerations and ways to minimize the potential risks from physical activity.
Health Benefits Of Physical Activity
The relationship between physical activity and health outcomes has been examined extensively in a large number of epidemiologic studies, which are summarized in the 1996 Surgeon General’s report (U.S. Department of Health and Human Services, 1996). These studies have shown physical activity to be associated with numerous health benefits, including reductions in the risk of premature mortality, cancer, cardiovascular disease, hypertension, diabetes, and osteoporosis. The weight of evidence derived from epidemiologic studies, short-term intervention, clinical investigations, and randomized clinical trials now provides strong evidence that engaging in regular physical activity is one of the best ways to improve overall health.
Several methodologic approaches are used to distinguish between health benefits that are caused by physical activity and those that are merely associated with it. While there was concern in the past that these observed benefits were due to confounding factors or reverse causation, this now seems unlikely, given the increasingly sophisticated design of epidemiologic studies and the growing body of research using short-term clinical intervention studies and randomized trials of increased physical activity leading to significant improvements in high-density lipoprotein (HDL) cholesterol, blood pressure, insulin resistance, and, to a lesser extent, weight loss.
Reverse causation is the idea that because people with disease are less likely to be active than healthy people are, physical activity can appear to be more beneficial in studies than it actually is. However, researchers are now able to use advanced statistical methods to address confounding factors and thus disentangle the effects of physical activity from the effects of other lifestyle factors. In addition, researchers now collect detailed data that enable them to reduce the possibility of reverse causation, such as excluding people with preexisting disease from their analyses and then studying the effects of physical activity only in those who were healthy at baseline. This method, along with controlling for confounding factors, has allowed researchers to be more confident in their conclusion that physical activity is one of the best ways to improve one’s overall health. When these epidemiologic approaches are further supported by short-term studies that show improvements in risk factors for chronic disease in response to increased physical activity, the biologic response data add to the causal interpretation of epidemiologic findings.
Lower Risk Of Cancer
Colon Cancer
Colon cancer is the second leading cause of cancer related death in the United States. However, the risk of developing colon cancer can be reduced through a number of lifestyle factors, with physical activity being one of the most important. Among both men and women, high levels of physical activity may lower the risk of colon cancer by as much as 50% (Colditz et al., 1997). Although studies have not consistently used a standard measure of activity or defined exactly what constitutes a ‘high’ level of activity, a dose–response relationship has been observed consistently across a variety of study designs and populations. In addition, this relationship has been observed across a wide range of weights, which suggests that the effect of physical activity on colon cancer incidence is independent of the effect of obesity.
Although maintaining a high level of physical activity throughout life appears to impart the greatest protection against colon cancer, this does not mean that sedentary people cannot reap the benefits if they become active. In a hallmark study by Lee et al., men who were sedentary at baseline and became active during the study had a 13% lower risk of colon cancer than men who were sedentary at baseline but remained so (Lee et al., 1991). In addition, the level of activity needed to reduce colon cancer risk appears moderate. Data from at least two prospective studies, conducted by Giovannucci and Martinez, indicate that both men and women can lower their risk of colon cancer by simply engaging in moderate physical activity, such as brisk walking or stair climbing, for 1 h per day (Giovannucci et al., 1995; Martinez et al., 1997). For participants whose only recreational activity was walking, there was a dose–response relationship between risk and walking pace: the faster they walked, the lower their risk was. For each additional hour of brisk walking per week, risk was reduced by approximately 10%.
Several mechanisms have been proposed to explain the link between activity and colon cancer. First, vigorous physical activity may lessen the amount of time that it takes stool to pass through the colon, thereby minimizing contact between the colon wall and any potential carcinogens in the stool. Second, physical activity may reduce circulating levels of insulin, which is a growth factor for colonic epithelial cells. Finally, additional hypotheses suggest that physical activity may alter prostaglandin levels, improve immune function, and modify bile acid metabolism.
Breast Cancer
A woman’s risk of breast cancer depends largely on the amount of estrogen circulating in her body. Because physical activity is thought to lower cumulative lifetime exposure to circulating estrogens, researchers have long speculated that it might lower the risk of breast cancer. Numerous studies have examined this possibility, and although not entirely consistent, the majority of studies support a modest, inverse relationship between physical activity in adulthood and breast cancer. The IARC concluded that this was a causal link between lack of physical activity and increased risk of breast cancer (International Agency for Research on Cancer, 2002). Overall, the reduction in risk is approximately 20% for women who achieve the CDC guideline of 30 min of physical activity most days of the week. The strongest reduction in risk of premenopausal breast cancer (a 60% reduction) has been observed for women who attain this level of activity (approximately 4 h per week) from menarche through to their 40s (Bernstein et al., 1994).
Bernstein and Colditz have theorized that physical activity in early childhood might also affect breast cancer risk, mainly by delaying the age at which a girl starts her regular menstrual cycles (called menarche). Physical activity may delay menarche by interacting with the adrenaline system to reduce levels of circulating estrogens. In addition, girls who are physically active have less fat tissue, and this may also lead to delayed menarche. Early age at menarche (younger than 12 years) is an established risk factor for breast cancer (Hankinson et al., 2004).
Lower Risk Of Cardiovascular Disease
Hypertension
Hypertension is a major underlying cause of cardiovascular complications and mortality in the United States. Fortunately, though, it can be both prevented and treated with physical activity. Physical activity causes the blood vessels to dilate, allowing blood to flow through the arteries more readily. In addition, it helps remove low-density lipoproteins from the artery walls, thus widening them. Finally, activity can help with weight loss, which can, in turn, lower blood pressure.
Several studies have demonstrated the efficacy of physical activity in lowering blood pressure, with many supporting a dose–response relationship such that the risk of hypertension diminishes with increasing levels of activity. Perhaps even more important is that several clinical trials have shown moderate physical activity to be as beneficial as vigorous physical activity in lowering blood pressure.
Cholesterol Levels
Regular physical activity may influence the amount of HDL cholesterol in the blood. HDL cholesterol is often referred to as ‘good cholesterol’ because it keeps low-density lipoproteins (or ‘bad cholesterol’) from building up in the arteries and causing atherosclerosis.
A number of studies have shown that active men and women tend to have higher levels of HDL cholesterol than their sedentary counterparts. For example, in one such study, conducted among female recreational runners, Williams found that HDL levels increased steadily with the number of miles that women ran per week (Williams, 1996). Similar results have also been reported for more moderate activity. For example, Parkkari et al. reported that previously sedentary men were able to raise their HDL levels by walking during golf games two to three times a week during a 20-week intervention (Parkkari et al., 2000).
Coronary Heart Disease
Largely by lowering blood pressure and increasing HDL cholesterol in the blood, physical activity can substantially lower the risk of coronary heart disease. Many studies have shown that active people have a substantially lower risk of coronary heart disease than their sedentary counterparts and that there is a dose–response relationship between activity level and risk. In a 1990 meta-analysis by Berlin and Colditz, the pooled relative risk for coronary heart disease in men and women, comparing risk in the highest level of physical activity to that in the lowest, was 0.56 among those studies judged to be of high quality (Berlin and Colditz, 1990).
There are several practical implications from recent studies on activity and heart disease. First, data suggest that individuals do not need to train for marathons or spend hours at a health club in order to lower their risk of heart disease. In a 1999 study by Manson et al., women who walked briskly for at least 3 h a week received the same amount of protection against heart disease as women who exercised vigorously for at least 1½ h a week (Manson et al., 1999). Both groups were 30–40% less likely to develop heart disease than those who were sedentary. Second, it appears that individuals might be able to get the same cardiovascular benefits whether they engage in several short sessions of activity per day (for example, three 10-min sessions) or in one longer session per day (a 30-min session). Although there are few data to support this notion directly, the 1996 Surgeon General’s report notes that it is reasonable to expect the benefits of intermittent activity ‘‘to be similar to those of continuous activity.’’ Finally, data suggest that it is never too late in life for people to reap the benefits of a physically active lifestyle. In the 1999 Manson study noted above, sedentary women who became active had a lower risk of heart disease than sedentary women who remained inactive. The more active the women became, the lower their risk was.
Stroke
Characterized by the blockage of blood flow to the brain or bleeding in the brain, stroke is one of the leading causes of death and permanent disability in the United States. However, the risk of this condition can be reduced with regular physical activity, since being active has beneficial effects on many risk factors for stroke, including obesity, heart disease, diabetes, hypertension, and high blood cholesterol.
Although early studies were conducted almost exclusively in men and were not consistent in demonstrating a link between activity and stroke risk, more recent studies now suggest that activity lowers the risk of stroke in both men and women. In addition, these studies have shown that even moderate-intensity activity, like walking, can lower risk. For example, in a large prospective cohort study conducted by Hu et al., women who walked briskly (at a pace of at least 3 miles/h) for at least 1 h per week were 30% less likely to have a stroke than sedentary women were (Hu et al., 2000). Those who walked at even quicker paces had further reductions in risk.
Lower Risk Of Type 2 (Adult-Onset) Diabetes
Type 2 (adult-onset) diabetes is already a major health problem in the United States, and the situation is only expected to get worse. With rates of obesity soaring and physical activity on the decline, the global prevalence of type 2 diabetes is expected to double over the next 10 years. Increasing the prevalence of physically active lifestyles, however, could help halt this trend. The relationship between physical activity and type 2 diabetes has been studied in great detail, with the large majority of studies suggesting a modest protective effect of about 30% for regular moderate activity (Jeon et al., 2007). In addition, several findings have had particularly practical implications. For example, it has become clear that regardless of how much a person weighs, he or she can reduce the risk of diabetes by becoming physically active. This is extremely important for overweight people, who have a greatly increased risk of diabetes and can thus benefit most from the protection offered by activity. Also noteworthy is that people who are sedentary can lower their risk of diabetes by becoming more active. Although a large increase in activity provides the most protection, even a very modest increase will offer some protection. Finally, if it is done for an extended period of time each week, walking can be as protective against diabetes as vigorous activity is. In a large prospective cohort study conducted by Hu et al., women who walked briskly for 3 h a week reduced their risk of diabetes as much as women who exercised vigorously for 1½ h a week (Hu et al., 1999). The more time women spent walking, and the faster they walked, the less likely they were to develop the disease. Taken collectively, these findings suggest that, regardless of people’s current weight or activity level, they can lower their risk of type 2 diabetes by walking more frequently – or more quickly.
Several mechanisms have been proposed to explain this beneficial link between activity and type 2 diabetes. First, type 2 diabetes occurs when the pancreas does not produce enough insulin or when the body does not effectively use the insulin that is produced. Physical activity can improve the body’s response to insulin and thereby lower the risk of diabetes. Second, overweight people are more likely to develop adult-onset diabetes than people at a healthy weight, and activity is an effective means of weight control and weight reduction.
Lower Risk Of Osteoporosis
Osteoporosis occurs when the bones in the body lose so much mass and become so brittle that they are prone to fracture. Physical activity is a well-established means of protecting against this condition. When a person is physically active, it places mechanical stress on the bones, forcing the tissue to absorb calcium and become stronger. In this way, physical activity directly promotes the building of bone. However, it also strengthens the bone tissue indirectly, by stimulating the muscles that surround bone tissue. As these muscles become larger and stronger, they place increasing pressure on the bone. This pressure stimulates the bone tissue to absorb calcium and grow in strength. Notably, the only bones protected by physical activity are those that are stressed during the activity. For example, walking will place stress on the bones of the spine and hips, but it will have no impact on the wrist.
Numerous studies have shown that being active early in life can have a long-term effect in preventing osteoporosis. This is because activity during childhood promotes the accumulation of bone mass – and the more bone that is accrued early in life, the lower the chance is of developing osteoporosis later. While this is reassuring for those who exercised as children, it need not be frightening for those who did not: Being active in adulthood can also prevent osteoporosis by slowing the rate of bone loss.
While most studies have shown that weight training and vigorous activity (like running) are the most effective activities for preventing osteoporosis and subsequent fractures, recent data suggest that walking might be just as beneficial. In a large study of women over age 65, Cummings et al. (1995) found a 30% reduction in the risk of hip fracture among those who walked for exercise compared to those who did not. The farther women walked, the lower their risk was. In the Nurses’ Health Study population, Feskanich et al. (2002) found that the risk of hip fracture in postmenopausal women dropped 6% for each hour increase per week of moderate activity. Overall, hip fracture risk was 55% lower in the most active women compared to the least. Several small, randomized controlled trials have supported these results, showing greater bone mass among women who walked than among women who were sedentary.
Although physical activity has a beneficial effect on bone for most women, engaging in too much strenuous activity can lead to dangerously low levels of estrogen and subsequent bone loss.
Weight Control
Excess body fat is a growing problem in the United States, with the prevalence of obesity among U.S. adults having reached 30% by 2002 (National Center for Health Statistics, 2007). This is of major public health concern, given that obesity is a major cause of mortality in the United States, contributing to at least 300 000 deaths per year. In addition, it substantially increases morbidity, impairs quality of life, and accounts for about 9% of all U.S. health-care expenditures. Physical activity has long been proposed as a means to stem the epidemic of obesity, since it can lead to modest weight loss in overweight and obese adults and can also help adults to maintain their weight. The evidence for this was reviewed in a report released by the National Heart, Lung, and Blood Institute in 1998 (NHLBI, 1998).

In that report, data were reviewed from 12 randomized controlled trials that examined the link between physical activity and weight loss, independent of diet. Ten of the 12 trials reported a mean weight loss of 5.3 pounds (or 2.4% of body weight) for active participants, while two trials reported no weight loss. (The duration of the interventions ranged from 16 weeks to one year.) In addition, ten of the trials compared the effects of exercise alone with diet alone, and nine showed greater weight loss among the diet-alone group than the exercise-only group. Taken collectively, these data led the report authors to conclude that physical activity alone (in the form of aerobic exercise) can result in modest weight loss among overweight and obese adults, and that these effects are independent of the effects of caloric reduction through diet. If increased physical activity is combined with a reduced calorie diet, the effects on weight loss are greater than they are for either activity or diet alone.
In addition to its modest effects on weight loss, physical activity may play a role in weight maintenance. Although this has not been formally evaluated in randomized controlled trials, data from observational studies suggest that physical activity is related to less weight gain over time and less weight gain after smoking cessation in women. In addition, post hoc analyses of intervention studies have suggested that physical activity is a predictor of successful weight loss.
Improvements In Mental Health
According to the World Health Organization (WHO, 2001), mental disorders are one of the top five causes of lost years of healthy life in the world, and they are expected to represent an even larger proportion of disease burden in the future. Although people have long speculated that physical activity might help prevent or even treat mental disorders, it is only in the past 30 years that there has been scientific evidence to support this. Data from prospective studies indicate that physical activity can prevent the development of mental health problems and can also improve the mental health of those who report problems such as depression and anxiety. Currently, there are few data on the optimal frequency, duration, and intensity of activity needed to improve or sustain mental health. However, too strenuous a regimen may have detrimental effects, as indicated by the mood disturbances observed among overtrained competitive athletes.
Although the release of endorphins is often cited as the reason that activity improves mental health, there are a variety of other possibilities. First, physical activity provides a time-out from the stresses of everyday life, and this can obviously lead people to feel more relaxed and less anxious. Second, being active has been shown to enhance self-efficacy (or confidence in one’s ability to do things), and this feeling often runs counter to feelings of depression and anxiety. Finally, people are often active in social settings, such as health clubs or walking groups, and social interaction is known to promote psychological well-being.
Increased Length Of Life
Men and women who participate in regular physical activity tend to live longer than those who are sedentary, even if the activity they engage in is only moderate in intensity. This has been confirmed in a number of large prospective cohort studies. For example, in a 1993 study by Paffenbarger et al., men who walked at least 10 miles a week were 33% less likely to die during the 25-year study period than those who walked less than 3 miles a week (Paffenbarger et al., 1993). This study also provided critical evidence that the negative effects of a sedentary lifestyle are reversible: Men who took up moderate physical activity, even after being inactive for years, reduced their risk of dying during the study period by 23%.
Optimal Level Of Physical Activity For Overall Health
To derive the health benefits discussed above, epidemiologic evidence shows that individuals should engage in physical activity on a regular basis. But just how much activity is needed to derive these benefits? For most health outcomes, there appears to be a dose–response relationship, with no lower threshold. What this means is that in terms of health benefits, some activity is better than none, and until extreme levels are reached, more is generally better.
Given the mounting evidence that moderate physical activity confers many of the same health benefits as vigorous activity, many leading health organizations have adjusted their guidelines accordingly. For example, the Surgeon General now recommends that people expend at least 150 calories per day (or 1000 calories per week). An expenditure of this amount can be achieved by walking briskly for 30 min per day or by engaging in more vigorous activity for a shorter duration (for example, 15 min of running at a pace of 10 min per mile). Both the Centers for Disease Control and Prevention and the American College of Sports Medicine offer similar guidelines, advising at least 30 min of moderate activity on 5 or more days per week. While this amount will yield significant benefit, further increases in physical activity will confer additional benefits and can be obtained by increasing the intensity, frequency, or duration of activity.
Despite the feasibility of the Surgeon General’s guidelines on physical activity (as compared to previous recommendations for more vigorous activity), both adult and adolescent populations in the United States are remarkably sedentary. More than 60% of adults do not meet the Surgeon General’s guidelines as described above, including 28% who are not physically active at all. Statistics are equally alarming for adolescents: About 14% of young people in the U.S. report no recent physical activity, including that of light to moderate intensity. Obviously, this is of great public health concern and warrants immediate attention.
Strategies To Increase Physical Activity
Strategies to increase physical activity aim to alter one or more of the many factors that influence levels of activity. Using the ecological model of health behavior, Sallis and Owen (1999) have categorized these factors as follows:
- intrapersonal factors: factors that occur within the individual’s mind or body, including biological, cognitive, and behavioral factors;
- social environment factors: social and cultural factors that promote or discourage a given behavior;
- physical environment factors: factors within the natural environment (such as weather or geography) or constructed environment (such as the transportation system or infrastructure for recreation) that promote or discourage a given behavior.
Most intervention research in the area of adult physical activity has focused on intrapersonal and social environmental influences and has taken place within the health-care setting, worksite, and community. However, there is now a shifting focus toward interventions and policies that address the physical environment as well.
Health-Care Settings
Provider-based strategies offer the opportunity for individual counseling and education about physical activity. Although these strategies have been shown to lead to statistically significant increases in activity, the increases are often modest and relatively short-lived. In a review of seven randomized controlled trials, Simons-Morton et al. (1998) found that physical activity interventions in health-care settings led to significant increases in activity in five studies but long-lasting increases (of more than 6 months) in only two. These results may be due in part to the many barriers that providers face when attempting to counsel their patients about activity. Providers are often pressed for time during their brief appointments, and many may not believe that physical activity is an important priority for discussion. In addition, many lack effective counseling skills. Interventions that have attempted to improve these skills suggest small but positive effects on patients, with 7–10% becoming active on the advice of their providers (U.S. Department of Health and Human Services, 1996).
Increasingly, Web-based tools for supporting positive lifestyle changes are making their way into the clinical setting. While it is currently unclear how effective such interventions are, an increasing number of studies are beginning to assess their potential, both in the healthcare setting and beyond.
Worksites
In the past, many individuals engaged in regular physical activity as part of their jobs. For example, at the turn of the twentieth century, more than 50% of the U.S. population was employed in agriculture, one of the most physically demanding fields of occupation. Today, that figure is less than 20%, with most Americans now working in jobs that have few if any physical demands. Although it is very unlikely that current trends in job sedentariness will be reversed, worksites are still an important venue in which to increase physical activity levels, since many adults spend a large proportion of their waking time in the workplace.
To date, there is limited evidence on the effectiveness of worksite strategies to increase physical activity. This is best summarized by Dishman et al., who, after conducting a meta-analysis on the topic in 1998, concluded that ‘‘the typical worksite intervention has yet to demonstrate a statistically significant increase in physical activity or fitness. The few studies that have used an exemplary sample, research design, and outcome measure have also yielded small or no effects. The generally poor scientific quality of the literature on this topic precludes the judgment that interventions at worksites cannot increase physical activity or fitness, but such an increase remains to be demonstrated by studies using valid research designs and measures’’ (Dishman et al., 1998).
Community
Community-wide trials to increase physical activity evolved from the concept that population-based strategies are needed to achieve meaningful, large-scale change. However, most of the community trials conducted to date have attempted to promote physical activity in the same ways as the provider and worksite-based interventions described above: by educating and persuading individuals rather than by altering environmental factors or setting policies that would create new social norms around activity. While the results of these trials have been somewhat promising in terms of their feasibility and acceptability to community residents, they have, overall, yielded relatively modest results in terms of effectiveness.
Environment And Policy
Environmental and policy approaches to increasing physical activity have the potential to influence large segments of the population simultaneously and, therefore, can often be less costly (on a per capita basis) and more enduring than approaches that focus on convincing people to be more active. Rather than persuade individuals to change, environmental and policy approaches aim to make it easier for individuals to choose and maintain physically active lifestyles. They do this by changing social norms (for example, making it more acceptable to commute to work by bicycle or foot or to exercise during the lunch hour) or by changing the environment (for example, improving road and sidewalk conditions for pedestrians and cyclists or making workplace stairways as safe, well-lit, and accessible as elevators).
Given the inherent difficulties of evaluating a population-based approach to behavior change, there is little published data on the effectiveness of environmental and policy approaches to increasing physical activity. In a 1998 review of the topic, Sallis et al. found only seven published studies, with interventions ranging in complexity from the posting of simple signs encouraging the use of stairs to the opening of 14 publicly funded recreation centers in Belfast (Sallis et al., 1998). The reported effectiveness of these interventions ranged with their complexity, but most had methodological flaws that eventually precluded the authors from reaching firm conclusions about their efficacy.
Summary Of Strategies
Because the factors that influence physical activity range from the individual to the environment, efforts to shift the population distribution of activity upward will require emphasis on all of the intervention points mentioned above: health-care settings, worksites, communities, and environment. Although there is limited evidence on the effectiveness of each intervention point alone, experience with tobacco tells us that leaving components unattended will surely result in diminished success. The challenge before the public health community now is to develop a comprehensive approach to physical activity that targets individual and environmental barriers simultaneously.
Safety Issues
Although the benefits of physical activity are well established, the risks must also be considered. These include injuries, sudden cardiac events, and, for women, irregular menstrual cycles. In general, these risks are outweighed by the vast benefits of physical activity and can generally be reduced with simple steps.
Increased Risk Of Injury
The risk of injury depends largely on the type of activity being done and how often and intensely it is being performed. People who participate in activities that require repetitive motion often suffer from overuse injuries. For example, individuals who participate in overhead sports, like swimming, tennis, and baseball, may suffer from shoulder problems, whereas runners tend to have foot, ankle, and knee injuries. The risk of these types of injuries can be reduced by stretching the muscles sufficiently before and after exercising.
Activity-related injuries can also be caused by roadway accidents. For example, people who walk, run, bike, or skate may injure themselves in a collision with a motor vehicle or in a fall that results from an uneven road surface.
Increased Risk Of Sudden Cardiac Events
Though rare, heavy physical exertion can trigger chest pain and heart attacks, particularly in people who are habitually sedentary and who sporadically engage in vigorous activity. Those who maintain a regular exercise program are much less likely to experience sudden cardiac events and, as noted above, have a much lower risk of coronary heart disease and stroke. The risk of exercise induced cardiac events can be reduced by not undertaking physical activities that are well beyond one’s normal level of exertion.
Increased Risk Of Irregular Menstrual Cycles
At some point in their lives, most women will experience an irregular menstrual cycle. Women who are extremely active, however, may experience such irregularities more frequently. Several studies have shown that female athletes have increased rates of amenorrhea, a disorder that is characterized by the absence of menstrual periods for six or more months in a woman who has not yet gone through menopause. When a woman misses her menstrual periods for such an extended period of time, it means that she is not ovulating and has low levels of circulating estrogen. This can impair fertility and may lead to a decrease in bone mass.
Conclusion
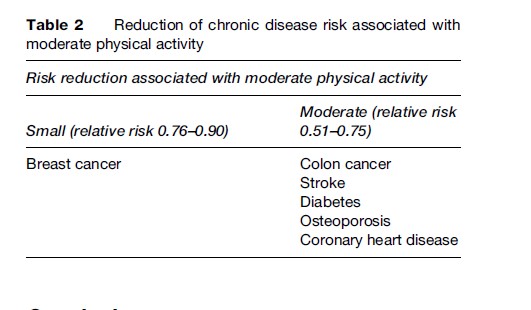
Overall, engaging in regular physical activity is one of the best ways to improve overall health. Although there are risks associated with activity, they are far outweighed by the long-term health benefits. Physical activity can prolong life, improve quality of life, and lower the risk of heart disease, stroke, diabetes, colon cancer, breast cancer, and osteoporosis (Table 2). In addition, it is an important component of weight management. Given that obesity is a major contributor to morbidity and mortality in the United States, the role of physical activity in preventing and treating this condition cannot be overestimated.
To achieve many of the health benefits described above, people need only to engage in moderate-intensity activity, like brisk walking, for at least 30 min on five or more days per week. What remains a challenge, however, is promoting this level of activity in a population that is predominantly sedentary. Although the most effective approach to doing this has yet to be determined, the public health experience with tobacco points to the need for a multifaceted approach that includes strategies aimed at both individual behavior change and environmental change.
Bibliography:
- Berlin J and Colditz G (1990) A meta-analysis of physical activity in the prevention of coronary heart disease. American Journal of Epidemiology 132: 612–628.
- Bernstein L, Henderson BE, Hanisch R, Sullivan-Halley J, and Ross RK (1994) Physical exercise and reduced risk of breast cancer in young women. Journal of the National Cancer Institute 86: 1403–1408.
- Colditz GA, Cannuscio CC, and Frazier AL (1997) Physical activity and colon cancer prevention. Cancer Causes and Control 8: 649–667.
- Cummings SR, Nevitt MC, Browner WS, et al. (1995) Risk factors for hip fracture in white women: Study of Osteoporotic Fractures Research Group. New England Journal of Medicine 332(12): 767–773.
- Dishman RK, Oldenburg B, O’Neal H, and Shephard RJ (1998) Worksite physical activity interventions. American Journal of Preventive Medicine 15(4): 344–361.
- Feskanich D, Willett W, and Colditz G (2002) Walking and leisure-time activity and risk of hip fracture in postmenopausal women. Journal of the American Medical Association 288(18): 2300–2306.
- Giovannucci E, Ascherio A, Rimm EB, Colditz GA, Stampfer MJ, and Willett WC (1995) Physical activity, obesity, and risk for colon cancer and adenoma in men. Annals of Internal Medicine 122: 327–334.
- Hankinson SE, Colditz GA, and Willett WC (2004) Towards an integrated model for breast cancer etiology: The lifelong interplay of genes, lifestyle, and hormones. Breast Cancer Research 6(5): 213–218.
- Hu F, Sigal R, Rich-Edwards J, et al. (1999) Walking compared with vigorous physical activity and risk of type 2 diabetes in women: A prospective study. Journal of the American Medical Association 282: 1433–1439.
- Hu F, Stampfer M, Colditz G, et al. (2000) Physical activity and risk of stroke in women. Journal of the American Medical Association 283: 2961–2967.
- International Agency for Research on Cancer (2002) Weight Control and Physical Activity Vol 6. Lyon, France: International Agency for Research on Cancer.
- Jeon CY, Lokken RP, Hu FB, and van Dam RM (2007) Physical activity of moderate intensity and risk of type 2 diabetes: a systematic review. Diabetes Care 30(3): 744–752.
- Lee IM, Paffenbarger RS Jr., and Hsieh CC (1991) Physical activity and risk of developing colorectal cancer among college alumni. Journal of the National Cancer Institute 83: 1324–1329.
- Manson J, Hu F, Rich-Edwards J, et al. (1999) A prospective study of walking as compared with vigorous exercise in the prevention of coronary heart disease in women. New England Journal of Medicine 341: 650–658.
- Martinez ME, Giovannucci E, Spiegelman D, Hunter DJ, Willett WC, and Colditz GA (1997) Leisure-time physical activity, body size, and colon cancer in women. Nurses’ Health Study Research Group. Journal of the National Cancer Institute 89: 948–955.
- National Center for Health Statistics (2007) Prevalence of Overweight and Obesity Among Adults: United States, 1999–2002. Hyattsville, MD: NCHS. http://www.cdc.gov/nchs/products/pubs/pubd/ hestats/obese/obse99.htm#Table%20 (accessed December 2007).
- NHLBI (1998) Clinical guidelines on the identification, evaluation, and treatment of overweight and obesity in adults – The Evidence Report. Journal of Obesity Research 6(2): 51S–209S.
- Paffenbarger R Jr, Hyde R, Wing A, Lee I-M, Jung D, and Kampert J (1993) The association of changes in physical activity level and other lifestyle characteristics with mortality among men. New England Journal of Medicine 328: 538–545.
- Parkkari J, Natri A, Kannus P, et al. (2000) A controlled trial of the health benefits of regular walking on a golf course. American Journal of Medicine 109(2): 102–108.
- Sallis J and Owen N (1999) Physical Activity and Behavioral Medicine Vol 3. Thousand Oaks, CA: SAGE Publications Ltd.
- Sallis JF, Bauman A, and Pratt M (Nov 1998) Environmental and policy interventions to promote physical activity. American Journal of Preventive Medicine 15(4): 379–397.
- Simons-Morton DG, Calfas KJ, Oldenburg B, and Burton NW (1998) Effects of interventions in health care setting on physical activity or cardiorespiratory fitness. American Journal of Preventive Medicine 5(4): 413–430.
- S. Department of Health and Human Services (1996) Physical Activity and Health: A Report of the Surgeon General. Atlanta, GA: US Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion.
- Williams PT (1996) High-density lipoprotein cholesterol and other risk factors for coronary heart disease in female runners. New England Journal of Medicine 334(20): 1298–1303.
- World Health Organization (2001) The World Health Report 2001 – Mental Health: New Understanding, New Hope. Geneva, Switzerland: WHO.
See also:
Free research papers are not written to satisfy your specific instructions. You can use our professional writing services to buy a custom research paper on any topic and get your high quality paper at affordable price.
ORDER HIGH QUALITY CUSTOM PAPER

Always on-time

Plagiarism-Free

100% Confidentiality



