
This sample Risk Communication Research Paper is published for educational and informational purposes only. If you need help writing your assignment, please use our research paper writing service and buy a paper on any topic at affordable price. Also check our tips on how to write a research paper, see the lists of health research paper topics, and browse research paper examples.
Risk communication, an essential function of public health, involves the effective and accurate exchange of information about health risks and hazards – often during a crisis or emergency – that advances risk awareness and understanding and promotes health-protective behaviors among individuals, communities, and institutions. Although forged through decades of applied experience in response to infectious disease outbreaks, industrial accidents, and natural disasters, contemporary public health risk communication principles and practices build upon a foundation of behavioral, health, and social sciences theory and research. Equally important, public health risk communication is increasingly an integral part of broad-reaching emergency preparedness activities. In this role, public health risk communicators (1) facilitate interactions between first responders and other stakeholders, (2) develop response plans and information dissemination strategies coordinated across diverse local, regional, national, and international agencies, (3) construct preparatory and advisory messages that reflect the diverse needs of potential audiences, and (4) identify the most effective and viable channels for delivering such messages during an emergency. More recently, many public health risk communication principles and practices have been proving instrumental to pursuits in noncrisis contexts such as health care and health promotion, thus broadening their application considerably.
The Emergence Of Public Health Risk Communication
Throughout the history of public health, effectively communicating about health risks with a broad range of constituents has proven a fundamental and enduring challenge. John Snow, for example, faced local officials who were ‘‘reluctant to believe’’ his claim that the epicenter of the 1854 cholera outbreak in London was the Broad Street water pump, and he secured their permission to remove the pump handle only on an experimental basis. Similarly, communication efforts to contain the spread of HIV in the United States met strident resistance from health care, public health, and community constituents.
More recently, unprecedented crises and emergency events occurring around the world (e.g., the 2004 Indian Ocean/Asian tsunami) have highlighted public health risk communication shortcomings that mitigated mobilization and coordination of public health resources, ‘‘undermined public trust and compliance, and unnecessarily prolonged economic, social, and political turmoil’’ (WHO, 2005: 1). Indeed, as Edward Baker, Assistant U.S. Surgeon General, observed:
the major public health challenges since 9/11 were not just clinical, epidemiological, technical issues. The major challenges were communication. In fact, as we move into the 21st century, communication may well become the central science of public health practice. (qtd. in Galvez et al., 2007)
Contemporary public health risk communication principles and practices have emerged over the last 50 years in response to such challenges; first from natural, industrial, and environmental disaster management, then as an integral component of health promotion endeavors targeting infectious and chronic disease prevention and management, and most recently in response to the threat of terrorism. Although there are distinct literatures detailing the unique application of risk communication to each of these public health contexts, several commonalities and generalizations are evident.
Public Health Risk Communication
Public health risk communication entails the systematic dissemination of information to diverse audiences (e.g., individuals, communities, institutions) facilitating their informed, independent decision making about the existence, nature, and/or severity of risks and hazards affecting health, safety, and the environment. Working under circumstances fraught with uncertainty, confusion, and a sense of urgency, public health risk communication practitioners must communicate with constituencies in ways that build, maintain, and/or restore trust and credibility while also persuading individuals to enact self-protective behaviors that will minimize adverse health outcomes.
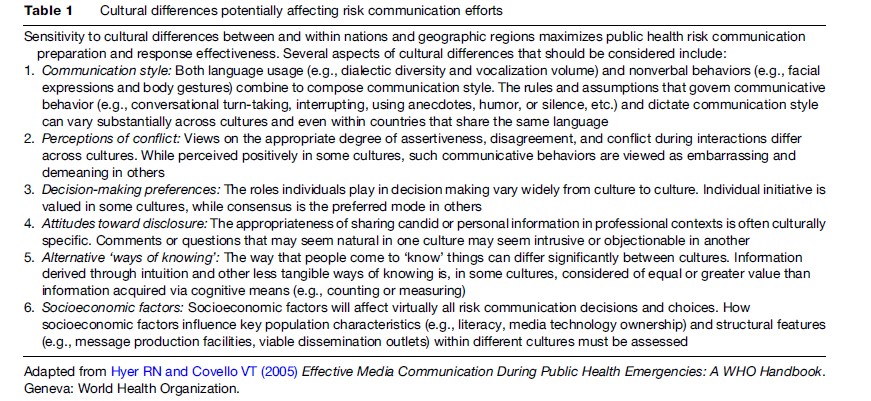
Public health risk communication messages, in other words, must convey to diverse audiences accurate and objective knowledge about and understanding of the health-affecting risk or hazard. To achieve maximum effectiveness, however, public health risk communication messages must also reflect local relevance and cultural competence, engender cooperation, and encourage constructive dialogue. Table 1 outlines several important considerations that should be integrated into public health risk communication messages for diverse audiences.
The Mass Media And Public Health Risk Communication
Equally important is recognition of the pivotal role frequently played by the mass media in distributing public health risk communication messages and, consequently, their potential influence on subsequent events. This fact is emphasized by the range of major public health organizations (e.g., Thesenvitz, 2000; U.S. Department of Health and Human Services, 2002; World Health Organization, 2005; Agency for Toxic Substance and Disease Registry, 2007; Centers for Disease Control and Prevention, 2007) that have published extensive guidelines and recommendations for involvement of the media during crises and emergencies.
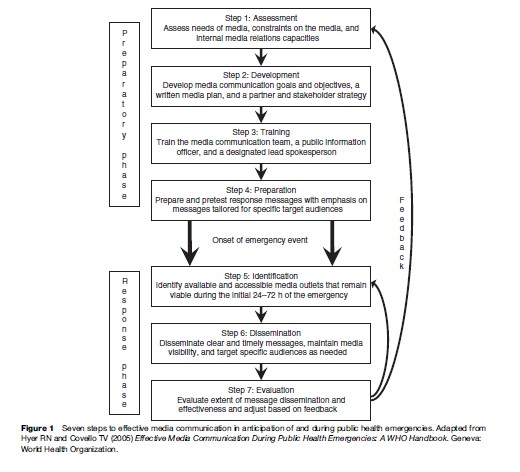
The World Health Organization handbook, Effective Media Communication During Public Health Emergencies (Hyder and Covello, 2005), offers a particularly comprehensive summary organized around a seven-step model. This model of effective media communication during public health emergencies is illustrated in Figure 1. As can be seen, the first four steps of the model detail ongoing preparatory activities (i.e., needs assessment, strategy development, response training, and message preparation) that public health risk communicators should undertake in anticipation of a potential emergency. The next two steps – identification of accessible media outlets and execution of message dissemination plans – are initiated once an emergency event is forthcoming or is rapidly evolving. The seventh step is evaluation. As illustrated in Figure 1, the evaluation step involves two feedback loops, indicating that evaluative activities should occur both as an ongoing activity during the emergency and, more substantially, following resolution of the event.

The necessity for public health risk communicators to evaluate continually the role played by mass media during an emergency was demonstrated during the 2005 Atlantic Hurricane Katrina, which devastated coastal areas of Alabama, Louisiana, and Mississippi. Essentially all strategic hurricane response planning for the region heavily involved traditional electronic media (e.g., radio and television broadcast stations and cable television systems) and emerging technologies (e.g., e-mail) as the primary emergency information dissemination channels. The magnitude of storm damage and subsequent flooding, however, virtually silenced all of these media, forcing public health risk communicators to seek alternative channels. Risk communication specialists in the Joint Information Center at the Centers for Disease Control and Prevention in Atlanta quickly recognized that the planned channels for message dissemination were inaccessible and turned to alternative mechanisms. Within days, for example, crucial health protective messages, printed in Atlanta and trucked to devastated areas, began reaching many of the most affected victims. Then, in the ensuing weeks, CDC staff who were deployed just outside the worst affected areas used the Internet and local facilities to print materials that were circulated among storm survivors at reentry and evacuation points, food and ice distribution centers, and door to door.
Risk Perception And Public Health Risk Communication
A growing interdisciplinary literature informs our understanding of how individuals perceive and respond to public health risk communication. In particular, research has focused on the cognitive mechanisms through which individuals are exposed to and attend to information about risk, how they interpret risk information in relation to themselves, and whether and how they act upon risk information to enact self-protective behaviors. Risk perception, defined as the subjective assessment or judgment of a threat, has emerged as a key concept. Indeed, risk perception, not the actual risk posed by a threat, seems the primary factor guiding cognitive, emotional, and behavioral reactions elicited when conditions challenge an individual’s health and safety. Lay and technical audiences, for instance, often perceive risk estimates quite differently. Consider a circumstance in which public health officials innumerate the likelihood of a health risk as 1 in 1000. Health experts understand this estimate in terms of relative risk; one person in every 1000 people is at risk. For the public, however, such estimates are commonly misinterpreted. Nontechnical audiences, in particular, tend to personalize health assessments, and their perceptions of risk often are distorted by an emotional bias emanating from concerns that individuals close to them are at significant risk.
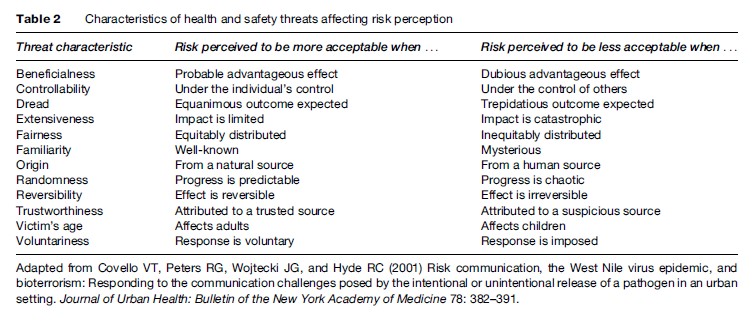
A range of factors has been identified that mediate risk perception. Specific characteristics of health or safety threats, for example, can influence how risks are perceived. Some of these characteristics, along with attributes shaping the directionality of perceived risk, are presented in Table 2. As an illustration, consider a health communication campaign, targeted at parents of asthmatic children, promoting home environment exposure-management awareness. Articulating multifaceted approaches involving direct actions (e.g., using dust-mite-impermeable bedcovers, avoiding tobacco smoke, damp-mopping hard surfaces) that parents can control, that they can voluntarily implement, and that predictably yield beneficial effects (National Institutes of Health, 2007) should help lower their perceptions of home environment asthma risks. Similarly, several social and psychological factors appear to diminish individuals’ comprehension of scientific or probabilistic information about risks to health and safety. For example, while elevated risk perceptions can sometimes promote proactive protective behaviors, they can also produce an unintended consequence: a contradictory effect engendering negative emotional reactions and creating resistance to health-protective recommendations and other risk-reduction messages.
Theoretical Diversity In Public Health Risk Communication
Strategies for overcoming social and psychological barriers to effective public health risk communication emerge from a number of theoretical perspectives. The mental models approach (Morgan et al., 2002), for example, offers tools for better understanding how a lay audience’s cognitive beliefs about medical and environmental risks impact their interpretations of health risk messages and outlines specific ways in which technical and scientific concepts can be tailored and focused into understandable risk communication. Specifically, the mental models approach involves a five-step method for creating and testing risk messages. The first step involves creation and analysis of an ‘expert model,’ which is depicted as an influence diagram, summarizing scientific evidence and expert opinion about a health threat. In step two, open-ended interviews of lay respondents assessing their beliefs about the health threat are undertaken to determine the external validity of the expert model. A confirmatory questionnaire, built upon information gleaned in the first two steps, is administered in step three to a large sample from the anticipated target audience in order to establish the population prevalence of health-threat beliefs. In step four, based on the accumulated results, risk communication messages designed to enhance awareness of and correct distorted beliefs about the health threat are developed and subjected to expert scrutiny. Further refinement of the health-threat risk communication messages using various evaluative research methods is the focus of step five. Growing evidence suggests that the mental models approach, when properly used, can yield clear and understandable messages about health risks.
Concepts from the health belief model ( Janz et al., 2002) can also inform public health risk communication practice. Within this framework, people are seen as engaging in self-protective actions to reduce health risk exposure if they believe they are vulnerable, believe that such actions will beneficially reduce their risk susceptibility, and believe that the barriers (or costs) of self-protective action are exceeded by the perceived benefits. Protection motivation theory, stages of change models, and other promising concepts (i.e., mental noise, negative dominance, and trust determination) have also informed public health risk communication practice.
Emerging Trends In Public Health Risk Communication
Advancements in our understanding of factors that can maximize the effectiveness of public health risk communication principles and practices continue throughout the behavioral, health, and social sciences. One emerging trend in public health risk communication is the development and implementation of effective individual-level risk communication strategies and messages. Although science-based evidence about the risk factors associated with chronic diseases and ill health has grown substantially, realization of the full benefits of this actionable knowledge can occur only when effective interventions are identified and when health professionals become proficient risk communicators. A number of recent systematic reviews illustrate, in fact, considerable efficacy of risk communication interventions (e.g., improving women’s health and outcomes following genetic testing and counseling) in clinical health practice settings (Edwards et al., 2000; Rowe et al., 2002; Butow et al., 2003).
What to do about the Internet and other new ‘communication technologies’ also remains an emerging issue facing public health risk communicators. Undoubtedly, the Internet offers a highly efficient channel for rapid dissemination of health and safety risk information. Effectively integrating the Internet into emergency response communication plans remains a challenge, however. Events surrounding the April 16, 2007, tragedy on the Virginia Polytechnic Institute and State University campus in the U.S. provide a vivid example. Following an early morning double-murder shooting in a campus dormitory, university officials relied primarily on e-mails to disseminate warning and advisory news and information to the university community. The initial notification, emailed over 2 h after the attack and several min after the day’s classes had begun, informed of an ongoing homicide investigation, urged vigilance and caution, and directed students and employees to a website for further updates. Only moments later, the deadliest shooting rampage on a U.S. university campus began. In this instance, the delayed timing of the Internet notification, the transitory nature of the target audience and, consequently, their limited e-mail access, and the dynamic nature of the emergency converged, essentially mitigating the effectiveness of the risk communication effort.
Finally, an emerging focus area where considerable progress is evident involves the practice of public health risk communication during crisis or emergency events. Crisis and emergency risk communication (CERC; Reynolds and Seeger, 2005), for example, is a systematic approach to catastrophe-bound public health risk communication that is broader and more comprehensive than traditional models. Foundational to the CERC framework is recognition that crisis and emergency events, while unpredictable, typically evolve through unique developmental stages, from pre-crisis to initial event through maintenance to resolution and on to evaluation. By projecting emergency events as developing in an orderly and sequential progressive manner, CERC promotes strategic anticipation of the information demands and exigencies of affected audiences during each catastrophe stage and highlights the essential preparatory work and event-bound practices necessary to satisfy anticipated risk communication needs.
Bibliography:
- Agency for Toxic Substance and Disease Registry (2007) A Primer on Health Risk Communication: Principles and Practices. Atlanta, GA: Centers for Disease Control and Prevention. http:// www.atsdr.cdc.gov/risk/riskprimer/index.html (accessed November 2007).
- Butow PN, Lobb EA, Meiser B, Barratt A, and Tucker KM (2003) Psychological outcomes and risk perception after genetic testing and counseling in breast cancer: A systematic review. Medical Journal of Australia 178: 77–81.
- Centers for Disease Control and Prevention (2007) Emergency Risk Communication: Overview. Atlanta, GA: Centers for Disease Control and Prevention. http://www.bt.cdc.gov/erc/index.asp (accessed November 2007).
- Edwards A, Hood K, Matthews E, et al. (2000) The effectiveness of one-to-one risk-communication interventions in health care: A systematic review.
- Medical Decision Making 20: 290–297. Galvez MP, Peters R, Graber N, and Forman J (2007) Effective risk communication in children’s environmental health: Lessons learned from 9/11. Pediatric Clinics of North America 54: 33–46.
- Hyer RN and Covello VT (2005) Effective Media Communication During Public Health Emergencies: A WHO Handbook. Geneva, Switzerland: World Health Organization. http://www.who.int/csr/ resources/publications/WHO%20MEDIA%20HANDBOOK.pdf (accessed November 2007).
- Janz NK, Champion VL, and Strecher VJ (2002) The health belief model. In: Glanz K, Rimer BK, and Lewis FM (eds.) Health Behavior and Health Education: Theory, Research, and Practice, 3rd edn., pp. 45–66. San Francisco, CA: Jossey-Bass.
- Morgan MG, Fischhoff B, Bostrom A, and Atman CJ (2002) Risk Communication: A Mental Models Approach. Cambridge, UK: Cambridge University Press.
- National Institutes of Health, National Asthma Education and Prevention Program (2007) Expert Panel Report 3: Guidelines for the Diagnosis and Management of Asthma; Full Report 2007. Bethesda, MD: National Institutes of Health. http://www.nhlbi.nih.gov/guidelines/ asthma/index.htm (accessed November 2007).
- Reynolds B and Seeger MW (2005) Crisis and emergency risk communication as an integrative model. Journal of Health Communication 10: 43–55.
- Rowe RE, Garcia J, Macfarlane AJ, and Davidson LL (2002) Improving communication between health professionals and women in maternity care: A structured review. Health Expectations 5: 63–83.
- Thesenvitz J (2000) Developing your messages: It’s a risky business. The Update, S1–S8. Toronto, Canada: The Health Communication Unit, Centre for Health Promotion, University of Toronto. http://www. thcu.ca/infoandresources/newsletters/fall2000suppfinal.pdf (accessed November 2007).
- US Department of Health and Human Services (2002) Communication in a Crisis: Risk Communication Guidelines for Public Officials. Washington, DC: Department of Health and Human Services.
- World Health Organization (2005) WHO Outbreak Communication: WHO Handbook for Journalists; Influenza Pandemic. Geneva, Switzerland: World Health Organization. http://www.who.int/csr/ don/Handbook_ influenza_pandemic_dec05.pdf (accessed November 2007).
- Albarrancı´n D, McNatt PS, Klein CTF, Ho RM, Mitchell AL, and Kumkale GT (2003) Persuasive communications to change actions: An analysis of behavioral and cognitive impact in HIV prevention. Health Psychology 22: 166–177.
- Bennett P and Calman K (eds.) (2001) Risk Communication and Public Health. Oxford, UK: Oxford University Press.
- Berry DC (2004) Risk, Communication and Health Psychology. Berkshire, UK: Open University Press.
- Braithwaite D, Emery J, Walter F, Prevost AT, and Sutton S (2006) Psychological impact of genetic counseling for familial cancer: A systematic review and meta-analysis. Familial Cancer 5: 61–75.
- Covello VT (2005) Risk communication. In: Frumkin H (ed.) Environmental Health: From Global to Local, pp. 988–1009. San Francisco, CA: Jossey-Bass
- Devos-Comby L and Salovey P (2002) Applying persuasion strategies to alter HIV-relevant thoughts and behaviors. Review of General Psychology 3: 287–304.
- Edwards A, Elwyn G, Covey J, Matthews E, and Pill R (2001) Presenting risk information: A review of the effects of ‘framing’ and other manipulations on patient outcomes. Journal of Health Communication 6: 61–82.
- Edwards A, Unigwe S, Elwyn G, and Hood K (2003) Effects of communicating individual risks in screening programmes: Cochrane systematic review. British Medical Journal 327: 703–709.
- Finnegan JR Jr and Viswanath K (2002) Communication theory and health behavior change: The media studies framework. In: Glanz K, Rimer BK, and Lewis FM (eds.) Health Behavior and Health Education: Theory, Research, and Practice, 3rd edn., pp. 361–388. San Francisco, CA: Jossey-Bass.
- Glik DC (2007) Risk communication for public health emergencies. Annual Review of Public Health 28: 33–54.
- Lipkus IM (2007) Numeric, verbal, and visual formats of conveying health risks: Suggested best practices and future recommendations. Medical Decision Making 27: 696–713.
- Lundgren RE and McMakin AH (2004) Risk Communication: A Handbook for Communication Environmental, Safety, and Health Risks, 3rd ed. Columbus, OH: Battelle Press.
- Plough A and Krimsky S (1987) The emergence of risk communication studies: Social and political context. Science, Technology, and Human Values 12: 4–10.
- Rogers RW and Prentice-Dun S (1997) Protection motivation theory. In: Gochman DS (ed.) Handbook of Health Behavior Research I: Personal and Social Determinants, pp. 113–132. New York: Plenun Press
- Rothman AJ and Salovey P (1997) Shaping perceptions to motivate healthy behavior: The role of message framing. Psychological Bulletin 121: 3–19.
- Rowe RE, Garcia J, Macfarlane AJ, and Davidson LL (2002) Improving communication between health professionals and women in maternity care: A structured review. Health Expectations 5: 63–83.
- Sandman PM (1989) Hazard and outrage in the public perception of risk. In: Covello VT, McCallum DB, and Pavlova MT (eds.) Effective Risk Communication: The Role and Responsibility of Government and Nongovernment Organizations, pp. 45–49. New York: Plenum
- Shilt R (1988) And the Band Played On: Politics, People, and the AIDS Epidemic. New York: St. Martin’s Press.
- Summers J (1989) Soho: A History of London’s Most Colourful Neighborhood. London: Bloomsbury.
- Ulmer RR, Sellnow TL, and Seeger MW (2007) Effective Crisis Communication: Moving from Crisis to Opportunity. Thousand Oaks, CA: Sage.
- Weinstein ND and Sandman PM (2002) The precaution adoption process model. In: Glanz K, Rimer BK, and Lewis FM (eds.) Health Behavior and Health Education: Theory, Research, and Practice, 3rd edn., pp. 121–143. San Francisco, CA: Jossey-Bass.
See also:
Free research papers are not written to satisfy your specific instructions. You can use our professional writing services to buy a custom research paper on any topic and get your high quality paper at affordable price.
ORDER HIGH QUALITY CUSTOM PAPER

Always on-time

Plagiarism-Free

100% Confidentiality


