
This sample School Health Promotion Research Paper is published for educational and informational purposes only. If you need help writing your assignment, please use our research paper writing service and buy a paper on any topic at affordable price. Also check our tips on how to write a research paper, see the lists of health research paper topics, and browse research paper examples.
Public Health And School
From a public health perspective, the promotion of positive health-related behaviors among children is critical to children’s health and well-being. A substantial proportion of adult morbidity and mortality is due to behavioral patterns established during childhood and adolescence, so public health interventions in these critical periods may yield lifelong benefits.
As almost all young people attend school throughout their childhood and adolescence, schools may provide an ideal setting for enhancing students’ health-related behaviors, health, and subjective well-being. Furthermore, school is the workplace for teachers, and their behavior and subjective well-being are of importance for the quality of their job and their motivation to get involved in tasks with health objectives. Health promotion in school can thus be seen to have three major objectives. First, promoting health and well-being among all representatives of the school community may be regarded as an important objective in itself. Second, by improving health and wellbeing, the intention is also to develop a good learning environment conducive to efficient teaching. The idea is that students who are satisfied with school and perceive themselves to have good health and a good quality of life will have a greater interest in, and potential to concentrate on, learning tasks in school. Similarly, teachers experiencing high job satisfaction and perceiving themselves to have good health and a good quality of life will have more energy to fulfill their teaching tasks in the best possible way. The third objective of health promotion in school addresses improving student skills in caring for their own, as well as others’, present and future physical, psychological, and social health.
Schools, however, do have competing priorities. For many, achieving academic success, and maintaining the commitment and discipline of students, is more important than meeting health-related objectives. Indeed, individual schools and the education sector as a whole have not always reacted positively to the perceived ‘exploitation’ by the health sector in the pursuit of health-related behavioral change and the well-being of students. To achieve progress in advancing both educational and health goals, greater attention needs to be given to a more holistic approach rather than the mere teaching of individual life skills. A more efficient and relevant approach may be to focus on those characteristics of the school environment that may have an impact on both academic achievement and school commitment, as well as an impact on health-related behaviors and subjective well-being.
Thus, the ultimate outcome of increased subjective well-being and behaviors conducive to health may be of relevance and interest to the educational aims of both general educators and health educators. Educators have an interest in health-compromising behaviors, as they tend to cluster with problem behaviors and alienation from school. Moreover, subjective well-being may be seen as an important prerequisite for learning and academic achievement in school. At the same time, academic coping may bolster adolescents’ self-esteem, which again may contribute to subjective well-being.
School Health Promotion
On the grounds presented above, school health programs aim at pursuing development of both health and learning among students. WHO aims in its Global School Health Initiative to promote the health of students, school staff, families, and other members of the community through schools. The initiative’s objective is to increase the number of ‘health-promoting schools,’ which are schools constantly strengthening their capacity as healthy settings for living, learning, and working. Regional networks of health promoting schools have been set up in Europe, Australia, the Western Pacific, and Latin America. These networks have identified certain strands of activities and approaches to meet the overall aims of a health-promoting school. The European Network of Health Promoting Schools has been in operation since 1992 and today involves over 40 countries in Europe. In its early phase, the network identified guidelines covering six areas that a health-promoting school should aspire toward:
- school health policies – this is a written document stating the aims the school is striving toward within its health-promoting effort;
- physical environment of the school – this should be safe and health-promoting;
- the social environment of the school – this should ensure a well-functioning and inclusive psychosocial climate for students and staff;
- school/community relationships – these should ensure close collaboration between the school and the local community to make the best of the competencies and resources available;
- the development of personal health skills – emphasis should be given for students to develop essential life skills to help them take care of their own as well as others’ physical, social, and mental health;
- school health services – this should be a crucial partner in the development of a health-promoting school.
In brief, these guidelines encourage schools that aspire to become health-promoting schools to develop programs that promote health, to extend their teaching beyond health knowledge and skills, to take account of the school social and physical environment, and to develop links with the community.
At later stages in the European Network, the promotion of staff health and well-being and the inclusion of health promotion in initial and ongoing teacher training have been highlighted. The overall principles follow WHO’s Ottawa Charter from 1985 through to the Jakarta declaration in 1997 including the principles of democracy, equity, and empowerment. The latter principle has been given particular emphasis as student involvement and development of students’ action competence are included as core elements in the development of personal health skills.
Similarly, and building on WHO’s Global School Health Initiative, the U.S. Centers for Disease Control and Prevention (CDC) has identified eight core components in its Comprehensive School Health Program:
- health education – a planned, sequential curriculum that addresses the physical, mental, emotional, and social dimensions of health;
- physical education – a planned, sequential curriculum that provides learning experiences in a variety of activity areas that all students enjoy and can pursue throughout their lives;
- health services – services provided by health professionals and available to students to appraise, protect, and promote health, including counseling and educational opportunities;
- nutrition services – access to a variety of nutritious and appealing meals that accommodate the health and nutrition needs of all students;
- counseling and psychological services – services provided by professionals to improve students’ mental, emotional, and social health;
- healthy school environment – the physical and aesthetic surroundings and the psychosocial climate and culture of the school that affect the well-being of students and staff;
- health promotion for staff – opportunities for the staff to improve their health status through health assessments, health education, and health-related fitness activities;
- family/community involvement – an integrated school, parent, and community approach for enhancing the health and well-being of students.
Both the WHO Europe and the CDC sets of principles and components for school health lean toward the combination of two major intervention strategies: (1) classroom education as an efficient vehicle for health education directed at developing personal health skills and influencing behavior and health, and (2) a supportive school environment that facilitates children’s and adolescents’ ability to cope with developmental tasks in a way that health-enhancing behaviors and well-being may be promoted. Inclusion of the second strategy is frequently considered essential to the definition of a ‘health-promoting school’ approach, or a ‘whole-school’ approach, as opposed to a set of health promotion activities without a unifying overall strategy. (The latter is sometimes referred to as ‘health education.’) The health-promoting school approach constituted school health policies and a joint effort by all staff and students across grades and classrooms. Emphasis is given to ‘bottom-up’ processes. A health-promoting school program requires that all the school stakeholders participate in identifying needs and engage in developing activities for change. Activities should be a result of negotiated decisions between staff and students and based on their goals and priorities for change. Some activities will take place in a specific classroom, whereas others will take place across classes and grades to create a whole-school experience around a project. If a school chooses to address change in an area where an existing evaluated approach exists, for example in a prepackaged design, this may be a preferred approach since it relies on materials and strategies already proven effective. But in a whole-school approach, this may be only one of many strategies chosen to fulfill overall aims for a health-promoting school initiative.
Relevance Of A Whole-School Approach
The reason why a whole-school approach is found to be important is that a supportive school environment may be considered a resource for the development of health-enhancing behaviors, health, and subjective wellbeing, while a nonsupportive school environment may constitute a risk. Within this perspective of resource/ risk, students’ satisfaction with school constitutes a key element, as previous research findings suggest a close association between students’ alienation from school and health-compromising behaviors.
Subjective well-being among students may be considered a relevant prerequisite for learning in the sense that it allows full concentration on the curricular tasks rather than on coping with distress. Promoting students’ satisfaction with school and their global well-being is a common goal for both educators and health promoters. For both of these groups, students’ satisfaction with school and global well-being are important goals in themselves. On the other hand, educators must also aim at enhancing students’ academic performance. Karasek and Theorell (1990) strongly assert that employers should regard job satisfaction as an important outcome in itself, and not only of interest as a means of increasing productivity. Such a statement is in line with how health promoters evaluate satisfaction with school.
Research into adult work environments has identified predictors of both job performance and job satisfaction, and has found that high autonomy and control, adequate demands, and high-level support from colleagues and management are key predictors (Karasek and Theorell, 1990). School may be considered students’ work environment. In this way, concepts from research on adults’ work environments may be relevant to models used to understand how students’ perceptions of school environments relate to their health behaviors and subjective well-being.
Positive experiences in the school environment may constitute a resource for academic achievement, satisfaction with school, and global subjective well-being among students (Samdal et al., 1998, 1999). Negative perceptions seem to represent a risk to these positive experiences, and appear to contribute instead to the development of health-compromising behaviors. In either case, the underlying mechanisms can be understood as related to meeting, or failing to meet, basic human needs and goals such as autonomy, social support, and coping with challenges (Ryan and Deci, 2001).
Studies have found that student autonomy is the most important facet of students’ psychosocial school environment (Samdal et al., 1998). Furthermore, it is the most important predictor of the dimension of students’ satisfaction with school, which is found to be the key associate of students’ academic achievement (Samdal et al., 1999). This finding corresponds to the results from research into the demand/control model in the adult work environment that indicate that employees can cope with high demands as long as they are given influence on and control in their work practices. In situations of high autonomy (and adequate demands), workers are also less likely to experience strain and depression, and thus higher levels of well-being are anticipated (Karasek and Theorell, 1990).
High-level support from fellow students has been found to be the facet of the school environment most strongly related to the subjective well-being of students. This finding corresponds well to research on social relationships, indicating that they may have a direct effect on subjective well-being (Ryan and Deci, 2001). Children and adolescents are in a developmental stage in which relationships with friends become increasingly important. School may therefore provide an important framework for these social relations through the function of providing a daily meeting place.
The focus on promoting positive development and experiences as opposed to preventing negative effect of stressful experiences represents in many ways a shift from the traditional public health focus on preventing disease to the new public health focus of promoting health and wellbeing. This shift is illustrated in Figure 1. The gray area represents gravity of present research and traditional focus in public health, whereas the white area suggests topics for future research and focus in new public health.
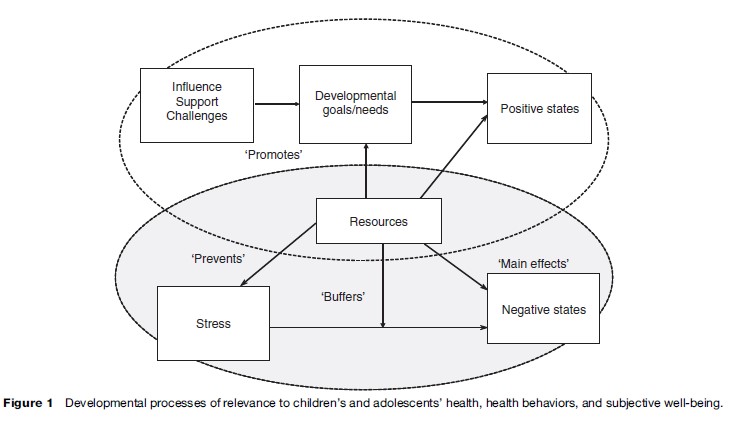
The traditional public health approach in school has been to identify resources in the psychosocial school environment that could prevent negative outcomes such as health-compromising behaviors, stress, subjective complaints, and mental health problems. Following the one-dimensional view of distress/well-being, the perspective has been that positive experiences in school may prevent stress perceptions and thus reduce negative outcomes and increase positive states. However, when considering recent research findings indicating that there might be different processes leading to negative affect states, new conceptual models are needed to understand the development of positive states as indicated by the white area in Figure 1. In this regard, the fulfillment of developmental goals seems relevant. Processes and activities that stimulate the intrinsically rewarding properties of agency (autonomy) and affiliation (social support) may be of particular interest. In this context, processes and activities taking place in the school setting may be highly relevant.
In the new public health approach, there is still a need to prevent development of health-compromising behaviors such as smoking and to develop health-promoting behaviors such as physical activity and healthy eating. Thus, health promotion in school is both about creating a supportive environment for development and learning, and about the traditional health education approach covered in subjects addressing the cross-curricular topic of health (e.g., physical education, home economics, biology, social science, and religion). With the aim of integrating health promotion into school policy, an important criterion will be to ensure that a systematic approach is taken by the whole school, thus avoiding health promotion in school that is solely dependent upon the individual teacher’s priorities for classroom activities. Part of the health-promotion activities should address long-term and general approaches used year after year, whereas other parts will have to deal with specific issues and problems arising throughout the year.
Effectiveness Of The Whole-School Approach And Single-Behavior/Topic Approaches
The whole-school approach is difficult to evaluate since a large number of complex components must be considered and all target groups must be included. Some evaluation studies do, however, show promising results indicating that a whole-school approach can positively impact staff development and the social climate of school and in some cases also positively influence health behaviors like healthy eating and physical activity (ListerSharp et al., 1999; Stewart-Brown, 2006).
Most interventions addressing improvement of health promoting behaviors are also found to be more promising when they include a whole-school approach rather than solely a health education classroom approach (ListerSharp et al., 1999). This applies to school-based mental health interventions (Wells, 2001; Licence, 2004) as well as physical activity and healthy eating programs. Physical activity interventions that include changes to the environment as well as organized recess activities seem more efficient than those that mostly use a curriculum approach through physical education (Sallis et al., 2003; Jago and Baranowski, 2004). Similarly, access to and availability of fruit and vegetables in the school setting is found to be of higher importance than changing attitudes in influencing eating behaviors (Blanchette and Brug, 2005).
Since little systematic evidence about the effectiveness of health-promoting, whole-school approaches on changing any single behavior exists, program evaluation becomes highly important for the developing field. Thus far, theory-driven programs have proven most successful. Many leading scholars therefore recommend that new programs be built on strong theoretical foundations.
Another important aspect to consider in evaluation of school health promotion programs is which parameters are the best measures of effectiveness. Thus far, health behaviors, health perceptions, and subjective well-being have been used as measurement of program effectiveness.
However, the 1to 3-year timelines of program implementation are short-term and may make relevant behavioral changes difficult to capture. Even more challenging are assessments of changes in school environments in the whole-school approach. Such complex, large-scale changes may take 6–8 years to achieve and identify (Green and Kreuter, 1999). Thus, two critical aspects must be considered. First, in short-term health promotion programs, changes in intermediate factors anticipated to influence health behaviors, health, and subjective well-being should be included as measures of effectiveness. Second, implementation time for school health programs should be extended. This, of course, also requires taking the long view when crafting the length of the funding scheme used to support the changes. Whole-school health promotion programs should be followed for at least 5–10 years, in order to identify and assess in adequate and rigorous ways the impact of the school environment changes on health behavior, health, and subjective well-being among students and staff.
Developing And Implementing School Health Promotion Programs
Successful implementation of a school health promotion program requires systematic planning and full engagement of target groups in order to inspire commitment, focus, and preparation to complete required tasks. Below follows an outline of the core elements of successful development and implementation of a school health promotion program.
The Development And Implementation Process
According to Fullan (1991, p. 65), implementation can be defined as ‘‘the processes of putting into practice an idea, a program, or a set of activities and structures, new to the people attempting or expected to change.’’ Implementation focuses on what happens in practice, and is concerned with the extent and nature of actual change, as well as the factors and processes that influence how and which changes are achieved (Fullan, 1991).
Four stages of implementation of programs have been identified (Green and Kreuter, 1999). The first stage addresses the motivation and role of the school leadership. As the leader of the school, the principal needs to make sure that the program is relevant to the school’s overall goals. Unless the principal and the rest of the school administration are convinced that the program is worthwhile, time and resources will be wasted and the program is unlikely to be fully or successfully implemented. In order to secure leadership motivation, schools should apply to participate, state their commitment to a minimum of 3 years for the implementation process, and describe how the project will be integrated in their school activities. A coordinator for the project should also be identified.
The second stage in the implementation process relates to formalization and institutionalization of the program. This means including the program in the school’s policy plan (or develop a policy or action plan if the school does not already have one), allocating time on the class and teacher schedules, and providing adequate resources and flexibility in the organization to facilitate necessary changes. Before formalization can take place, it is the responsibility of the principal to motivate and facilitate teachers’ participation in the program. Formalization of the initiative through allocation of time and resources demonstrates the school leadership’s motivation and priority and thus represents an important motivational factor for teachers’ commitment to the implementation of the initiative (Donaldson, 2001). Formalization becomes a way to set social norms among teachers.
In the health-promoting school approach, core elements of implementation are based on what the school aims to change or achieve. Identification of goals for change may be facilitated by use of a systematic planning tool suited to analyze both existing realities and developmental needs. The Precede-Proceed model developed by Green and Kreuter (1999) is such a tool. It focuses on the importance of identifying overall aims (what is to be achieved, and why this is important) before identifying actions that can meet the aims (how to achieve the aims). It is very important to allow adequate time for the planning phase to ensure that all needs are assessed and prioritized and to engage all participants. Survey tools and focus groups of students and staff may be useful in the needs assessment process. In addition, the identification of national forces and trends relevant to the local setting as well as national and international data on students’ health behaviors, health perceptions, and school satisfaction may constitute an important framework for identifying target areas. An example of such a data source is the European and North American Study of Health Behavior in School-Aged Children. A school may choose to address a problem or situation in a topic area where an effective program already exists. Use of a program with demonstrated efficacy may thus save valuable time and resources.
When the first and second steps of implementation have been achieved, this sets the stage for the third stepchange in teachers’ behavior and practice. These changes depend on the teachers’ motivation for and understanding of the initiative. The teachers will be the key implementers of the initiative for the students. Therefore their priority, conviction, and competence are vital to the initiative’s success.

The fourth and final stage involves change in student behavior, competencies, and experiences. Students’ change depends very much on how school administrators and teachers organize school and class activities. Moreover, much is gained when students are invited and trained to participate and claim a stake in school change.
All four stages involve a combination of bottom-up and top-down processes. The first two stages are very much top-down-driven by school leadership. However, initiatives are most successful when teachers and students are engaged as active participants in decision making. The third and fourth stages are more ‘bottom-up’ processes: Action is required from the key target groups. The point is that both bottom-up and top-down processes are necessary for success in the whole-school approach.
Although the four stages of change are presented as sequential phases, they are often parallel or cyclic in practice. The school leadership must continue setting priorities and advocating the initiative’s values if teachers are to sustain their commitment. Further, formalization needs to be given high focus as new strategies are developed and need to be integrated in the school organization. Finally, teacher and student behavior need continuous stimulation and facilitation in order to sustain changes over time. A case example presenting how one school worked its way through the four phases is provided in the following discussion.
Case Example
The case is set in a secondary school situated in a suburb of a major city in Norway. The school has three classes at each grade level. Forty percent of the students are immigrants. In this example, concrete actions were undertaken by the school according to four phases of development and implementation described in this research paper.
In the first phase, leadership motivation, the school’s leadership identified a ‘whole-school health promotion initiative’ as a way to achieve change. They anticipated that this approach would allow them to build on their established competencies, to collaborate with partners, and to use policy plans to achieve changes in practice. Further, a whole-school approach to health promotion also fits well with the school’s vision for its work:
This school is to be an active school where everyone is responsible for developing a good environment for learning and contributing to a high level of competence, and should also be a place where the students experience safety, satisfaction, and belonging.
The vision thus emphasizes both learning and the development of a supportive environment. Here exists a balance between these two priorities. On this foundation, school leaders decided to move the project forward by inviting the teaching staff to consider it and to brainstorm about how it might be implemented.
In the second phase, emphasis was given to anchoring health promotion aims and activities within the school’s policy plan. Health promotion was included as one of three strands of development in the school’s policy plan and ‘regular practice.’ The two other strands of development were ‘cultural elements’ and ‘academic improvement.’ The regular practice of the school includes social staff events, special activities for graduates, increased student involvement through the student council structure, and training in the use of information technology for the first-year students.
In identifying aims and relevant activities, the school used Green and Kreuter’s (1999) Precede-Proceed model. In line with the model, they asked themselves the following questions: (1) What are our current challenges? (2) What do we want to achieve? (3) Which actions do we need to take? and (4) How can we implement our actions?
In order to answer question (1), the school asked its university partner to conduct a survey to explore student and staff satisfaction with school as well as their health and health behaviors.
In response to question (2), the leadership invited students and the staff to prioritize areas identified in the survey. In this way, four areas or projects were named: (1) to improve the physical and psychosocial school environment, (2) to establish a cafeteria, (3) to reduce smoking, and (4) to increase physical activity levels.
In response to question (3), the school wanted to build on research that identified how physical surroundings influence behavior and well-being. Therefore, improvements in the school’s physical environment meant painting walls and decorating with art and flowers inside and outside. The aim was to improve the aesthetics and thereby enhance well-being and decrease vandalism. The school succeeded in its approach.
The establishment of a cafeteria served two purposes.
First, the aim was to provide options for students who did not pack their lunch (which is the common approach among Norwegian schoolchildren). The cafeteria made it possible for students to buy and eat healthier foods. Secondly, the cafeteria aimed to create a safe and pleasant meeting place for the students.
The aim of smoking cessation was addressed by introduction of a prepackaged program of proven efficacy.
Finally, to address the challenge of students’ physical activity, the school provided time and opportunities for student recess and after-school activities. Toward these ends, the school set aside additional staff hours to organize and supervise activities.
In response to question (4), behavior change among teachers was explored. This constituted phase three of the development and implementation process. Throughout the planning process, staff had been asked to identify visions and priorities. School leaders helped keep discussions focused and provided motivational cues for the whole-school health promotion approach. Two out of four of the school’s chosen foci did not involve teaching resources or teacher involvement. However, the two that did involve teachers were appropriately planned and prepared to engage their skills and attention. Before the school implemented the antismoking program, all teachers participated in a training program to review the program’s core principles and design. Also, teachers were actively engaged in planning and organization of physical activities in collaboration with a student group. Further, the time teachers spent in these activities was officially counted as ‘teaching hours.’
In the final phase, four years after initiation of the project, the school commissioned another survey to identify changes in student behavior. The survey showed that vandalism had stopped, more students ate lunch during the school day, smoking rates decreased, and students were more physically active. Moreover, the school observed a substantial decrease in sick leave among the staff.
Throughout the whole project, management played a key role in keeping the process focused. The school had identified a group in charge of the project’s development and activities. This group consisted of teachers, a parent, a representative from the police, and the school health nurse. School management and the project group chose to focus initially on actions that required only small changes in daily practice. Only after a couple of years into the process were more substantive changes introduced, for example, an hour set aside for free activities in the middle of the school day. For that change, the staff was asked to facilitate and supervise the hour in collaboration with student representatives.
The school worked extensively with other partners, particularly with the school nurse and the police. These partnerships were well-established prior to the project, but were strengthened through the work of the project. Management’s prioritization of the project provided important frameworks and incentives for its implementation and facilitated access to time and resources. Mutual planning time involving the whole staff was used to develop a platform for the project. An important part of the competence building and development of a mutual base was established through international visits to schools within the European Network of Health Promoting Schools. In this way, participants learned how others organized health promotion policies and practices.
Finally, the school leadership was well-trained in developing policy documents. Thus, they were quickly able to develop concrete objectives and actions. The policy document guided the practice of the school and was perceived as a text that united and inspired the staff. The deliberate use of the policy document to initiate and guide the school’s activities was crucial to its successful change.
Evaluation And Sustainability
The cyclical nature of the relationship between stages is evident in considerations of sustainability. Ongoing evaluation is required. The school must ensure its aims stay in focus. Evaluation is integral to building knowledge about what works. Thus, schools may gain much through collaborations with colleges and universities in terms of assessing and documenting efficacy.
Research suggests that collaborative school cultures and formalized implementation influence sustainability (Fullan, 1991). Green and Kreuter (1999) highlight the importance of continuous support and feedback. School leadership plays a significant role in this regard. In most implementation processes, resources and training are typically provided only in the initial phases. However, teachers’ commitment and skill building over time require allocation of resources for ongoing training.
Principals As Facilitators Of Implementation
School leadership, and in particular the principal, have a key role in the implementation and sustainability of school health promotion. The principal is central to creating the organizational conditions, capacity, and readiness required for successful implementation of an initiative. The capacity building aspect relates to time and resource allocation, competence development, and administrative structures and strategies designed to empower and involve teachers and students. The readiness-building aspect involves motivating and advocating a value basis for the initiative by linking it to the articulated overall aims of the school.
In their role as facilitators of interventions and innovations, school principals frequently concentrate on managerial and organizational aspects such as allocation of resources and time for the intervention. Research indicates that in order for school principals to be successful agents of intervention they also need to give emphasis to the leadership role. Leadership, however, does not replace management, but should be a facilitator of it (Daft, 1999). Leadership requires an awareness of a sustained long-term aim for the implementation, through building and maintaining a supportive organizational culture, establishing commitment to the goals and values of the program, and developing direction for the school in its work. Daft (1999) suggests three core elements in principals’ roles as they implement programs: to provide direction, to secure alignment, and to enable students and staff. Each of the elements includes leadership and management strategies, as presented next.
To Provide Direction
Implementation of programs involves the introduction of something new and thus requires change. Leadership means helping to direct that change by articulating a clear vision, setting priorities and developmental goals, and charting a plan to achieve these visions and goals. Leadership is supported by managerial approaches used to identify concrete, step-by-step actions, to allocate resources, and to schedule the program into the daily life of the school.
To Secure Alignment
Closely related to providing direction is the act of aligning the people involved in the program. In order for teachers to be willing to spend time and energy on the program, they need to be convinced of its utility. In the leadership role, the principal must communicate the vision and the values of the program to gain alignment and commitment. A crucial element in the alignment process is to build and nurture collaboration among the teachers. Supporting the leadership strategies, managerial actions integrate the program into the school’s written policy plan and thus make it a shared strategy that all teachers are committed to use. Formalization is also advanced by monitoring the extent to which teachers follow the school plan. Careful alignment around values and questions of relevance can influence teachers’ conviction of the program’s utility and thus decrease tensions they may experience as change occurs.
To enable
Finally, successful implementation also requires that the principal ensures that the teachers have the tools and training to use the program. In the leadership capacity, the principal needs to be available as a discussion partner for the teachers during implementation. The leader probes and listens to teachers to identify their needs and to give them feedback. In the management role, the allocation of resources and time for teacher training and program implementation (including teachers’ planning time) is crucial. Teacher training is critical to successful program implementation. In a new health promotion initiative, teacher training needs a broader focus than in a prepackaged program. In either case, the aim of collaboration between teachers, school leadership, and students is vital.
Leadership and management strategies are also important to secure the sustainability of the program. A long-term perspective on the three core elements of a principal’s role is important. Experience over time helps teachers identify any impact of the initiative on their daily teaching life and thus the program’s utility. The principal’s ongoing attention to how the program advances the school’s goals enhances sustainability. This attention helps teachers cope with changes and urges professional development. Further, the principal’s management strategies maintain the new program’s position in the overall school policy plan and thus allow for rational allocation of resources, particularly in the realm of ongoing teacher training and staff development.
Conclusions
In summary, effective school-health promotion should be based on systematic identification of what the school wants to achieve through the initiative. Often, it is wise and efficient to use an evaluated program of demonstrated efficacy. In other instances, a school may have to develop a unique program based on a comprehensive local needs analysis and assessment of resources. Activities should be built on existing theory and evidence of impact when available. It is also important in the whole-school approach to secure commitment of both students and staff. Activities and approaches should be planned to incorporate necessary changes in the physical and social environment of a school in addition to more traditional health education approaches aiming at improving students’ individual skills and attitudes. The school health service and other relevant collaborators should also be involved to ensure use of all available competencies and resources. School leadership has a crucial role to play in facilitating both development and implementation of the school health-promotion program. Moreover, evaluation of processes and outcomes is critical. Systematic development, implementation, and evaluation are required to advance deeper knowledge of what constitutes an effective school health-promotion program.
Bibliography:
- Blanchette L and Brug J (2005) Determinant of fruit and vegetable consumption among 6–12-year-old children and effective interventions to increase consumption. Journal of Human Nutrition and Dietetics 18: 431–443.
- Daft RL (1999) Leadership: Theory and Practice. Fort Worth, TX: Dryden Press.
- Donaldson GA (2001) Cultivating Leadership in Schools: Connecting People, Purpose, and Practice. New York: Teachers College Press.
- Fullan MG (1991) The New Meaning of Educational Change. London: Cassell.
- Green LW and Kreuter M (1999) Health Promotion Planning: An Educational and Ecological Approach. Mountain View, CA: Mayfield Publishing Company.
- Jago R and Baranowski T (2004) Non-curricular approaches for increasing physicalactivity in youth: A review. Preventive Medicine 39: 157–163.
- Karasek R and Theorell T (1990) Healthy Work: Stress, Productivity, and the Reconstruction of Working Life. New York: Basic Books.
- Licence K (2004) Promoting and protecting the health of children and young people. Child: Care, Health and Development 30(6): 623–635.
- Lister-Sharp D, Chapman S, Stewart-Brown S, and Sowden A (1999) Health promoting schools and health promotion in schools: Two systematic reviews. Health Technology Assessment 3(22): 1–207.
- Ryan RM and Deci EL (2000) Self-determination theory and the facilitation of intrinsic motivation, social development and well-being. American Psychologist 55(1): 68–78.
- Sallis JF, McKenzie TL, Conway TL, et al. (2003) Environmental interventions for eating and physical activity: A randomised controlled trial in middle school. American Journal on Preventive Medicine 24: 209–217.
- Samdal O, Nutbeam D, Wold B, and Kannas L (1998) Achieving health and educational goals through schools: A study of the importance of school climate and students’ satisfaction with school. Health Education Research 13(3): 383–397.
- Samdal O, Wold B, and Bronis M (1999) The relationship between students’ perceptions of the school environment, their satisfaction with school and perceived academic achievement: An international study. School Effectiveness and School Improvement 10(3): 296–320.
- Stewart-Brown S (2006) What is the evidence on school health promotion improving health or preventing disease and, specifically, what is the effectiveness of the health promoting schools approach? Report of the Health Evidence Network. Copenhagen, Denmark: WHO Regional Office for Europe. http://www.euro.who.int/ document/e88185.pdf (accessed October 2007).
- Wells J, Barlow J, and Stewart-Brown S (2003) A systematic review of universal approaches to mental health promotion in schools. Health Education Journal 103(4): 197–220.
- Blum RW, McNeely C, and Rinehart RM (2002) Improving the Odds: The Untapped Power of Schools to Improve the Health of Teens. Minneapolis, MN: Center for Adolescent Health and Development, University of Minnesota.
- Currie C, Roberts C, Morgan A, et al. (eds.) (2004) Young People’s Health in Context. Results from the 2001/2002 Survey in the Health Behavior in School-Aged Children Study. Copenhagen, Denmark: World Health Organization.
- Clift S and Jensen BB (2006) The Health Promoting School: International Advances in Theory, Evaluation and Practice. Copenhagen: Danish University of Education Press.
- Fullan MG (1992) Successful school improvement. Toronto, Canada: OISE Press.
- Tones K and Green J (2004) Health Promotion: Planning and Strategies. London: Sage Publications.
- WHO (1986) Ottawa Charter for Health Promotion: First International Conference on Health Promotion, Ottawa, Ontario, Canada, November 17–21.
- hbsc.org – Health Behaviour in School-Aged Children, a World Health Organization Collaborative Cross-National Study.
- cdc.gov/HealthyYouth/CSHP – National Center for Chronic Disease Prevention and Health Promotion, Healthy Youth! Coordinated School Health Program.
- who.int/school_youth_health/en/.
- who.int/school_youth_health/gshi – World Health Organization, School and Youth Health, Global School Health Initiative.
See also:
Free research papers are not written to satisfy your specific instructions. You can use our professional writing services to buy a custom research paper on any topic and get your high quality paper at affordable price.
ORDER HIGH QUALITY CUSTOM PAPER

Always on-time

Plagiarism-Free

100% Confidentiality


