
This sample Unemployment and Health Research Paper is published for educational and informational purposes only. If you need help writing your assignment, please use our research paper writing service and buy a paper on any topic at affordable price. Also check our tips on how to write a research paper, see the lists of health research paper topics, and browse research paper examples.
Introduction
Research during the recession of the 1930s and from the 1980s onward has provided strong evidence of an association between unemployment and various indicators of mental and physical health and causes of death in industrialized countries. Although poor health has also been observed among those exposed to job insecurity, much less work has been done in that area. This may be partly because there is less obvious reason to believe that job insecurity could affect health (unlike unemployment it involves no loss of income) and partly because large changes in the structure of the labor markets that have occurred only in the past 25 years have transformed both the experience of unemployment and job insecurity.
Major determinants of this labor market restructuring have been an increase in the service economy, technological innovation, globalization, and the major reorganization of services traditionally provided by the public sector. These structural changes have brought about shifts in labor market experiences. Many developed countries face persistently high levels of unemployment, and long-term unemployment has grown rapidly. Unemployment continues to be a major cause of low income, poverty, and marginalization, and with increasing length of unemployment the consequences of severance of social ties with the work community may be exacerbated. Furthermore, even in countries where unemployment rates are low, many workers, who previously thought they had a job for life, may now feel much less secure, and job insecurity has become more widespread in many Organization for Economic Co-operation and Development (OECD) countries since the mid-1980s.
In the world of rapidly changing labor market conditions, understanding the effects of unemployment and job insecurity on health continues to be an important concern for public health. However, although unemployment and job insecurity have been shown to have clear associations with health, the mere documentation of an association provides little information about the explanations that underlie these relationships. Most of the studies in this area of research have tried to assess the contribution of alternative explanations for the observed associations. Research into the health effects of unemployment and job insecurity contribute to the more general social epidemiological debate on the health effects of psychosocial stressors. For more than three decades job loss has been considered to be one of the most stressful life-events, coming close behind the highest ranking events: the death of close family members and family breakdown.
Explanatory Framework
The interpretation of the association of unemployment and job insecurity with health is complicated, and two broad types of mechanisms may form the basis for an explanation. These explanations are not exclusive of each other, but are likely to work in tandem.
- Causal effects of unemployment and job insecurity: Job insecurity, becoming jobless, and prolonged redundancy have negative effects on health and increase the risk of premature death. The causal effects are mainly assumed to be mediated through increased psychosocial stress and increased tobacco and alcohol consumption, as well as loss of income and material deprivation.
- Selection: Persons likely to work in insecure jobs, to become unemployed, or to have difficulty finding reemployment have preexisting ill health and/or lifestyle (e.g., tobacco and alcohol consumption, poor diet), socioeconomic (e.g., social class, housing tenure), or other personal characteristics (e.g., age, sex, physical weakness, psychological characteristics, and early life experiences) that increase the risk of future ill health and mortality. These preexisting factors have typically accumulated over a long period during the life course of these individuals.
The solid lines in Figure 1 show the pathways through which the causal effects of unemployment and job insecurity on health may be mediated. One of the main proposed intervening factors is psychological stress. Increasing job insecurity is likely to lead to worry about financial security and changes in work characteristics; actual unemployment may, for example, lead to deterioration of self-esteem, loss of respect from others, and loss of interpersonal contacts in the workplace. These in turn may affect health directly through biological pathways or health-related behaviors. The direct biological pathway may be through immune suppression or the functioning of the immune system in general. Another possible path is through changes in health behaviors that can be seen as attempts to cope with the psychosocial stress associated with job insecurity and job loss.
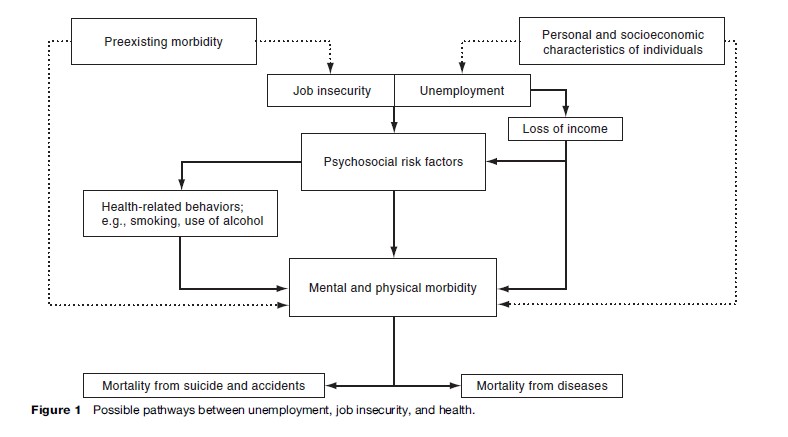
In the case of job loss – but of course not in the case of job insecurity – the decline of income and associated material hardship may also influence health. Such influences again may be associated with health-related behaviors, such as changes in diet, or with adverse changes in housing conditions and reduced access to medical care.
Selection may account for the association between unemployment and health in two different ways, which are depicted in Figure 1 with dotted lines. The most obvious form of selection is that preexisting ill health influences job insecurity and chances of unemployment (sometimes referred to as health-related selection or direct selection). The other possibility is that certain personal characteristics, such as mental instability or drinking problems, or socio-demographic characteristics, such as low education and social class, increase the likelihood of both job insecurity and unemployment, as well as increase the risk of ill health and mortality (this pathway is sometimes referred to as indirect selection).
The relative contribution of the different pathways is likely to vary according to the context in which job insecurity and unemployment are experienced. In particular, the level of unemployment and the social benefits that the unemployed receive may modify these health effects.
Study Designs And Data Sources
Because of the difficulties in unraveling the direction of causal relationships in aggregate and cross-sectional studies, we briefly present selected longitudinal studies that have been used at the individual level for disentangling the relationship of unemployment and job insecurity with health.
Longitudinal Follow-Up Studies Of Individuals
Several studies have investigated the relationship of unemployment and job insecurity with health through observational follow-up studies of individuals. Usually, in such studies the exposure (unemployment) and possible confounders (factors that may determine both unemployment and health) have been assessed at the baseline. The study population is then followed for health outcomes prospectively. Similar designs have been also used to study health changes after reemployment. These longitudinal study designs are very common in observational social epidemiology more generally.
However, strong causal inferences about the harmful effects of unemployment and job insecurity on health on the basis of observational follow-up studies are not always fully warranted because of the inadequate assessment of selection effects. Although selection based on preexisting ill health seems of lesser importance in this context, lack of data on personal characteristics and lifestyle makes it difficult to control for all possible selection factors. Factory closure and downsizing studies are able to overcome some of these problems.
Studies On Workplace Downsizing And Closure
Job insecurity and unemployment are not random events. However, in certain situations, for example at a time of very rapid downsizing or closure of workplaces, job insecurity and chances of being laid off increase for all employees, regardless of their individual characteristics. Such ‘natural experiments’ provide a powerful study design when random experimental allocation of subjects to exposure is impossible. A comparison of the ‘naturally’ exposed group to a not exposed reference group closely resembles a controlled experiment. This means there are no plausible selection processes involved, and such factors as poor health or age are not influential in increasing the risk of job loss. Inferences about causality are strong under such conditions.
The ideal factory closure study should have data from a period of secure employment and a control group of participants who remain employed in a similar factory throughout the study follow-up period. Obviously, opportunities to perform such studies are rare, and even when they do occur the number of workers involved is usually insufficient to detect effects on relatively rare outcomes. An added and often difficult-to-quantify problem with factory closure studies is that rumors of closure may circulate in the period leading to the closure. Employees who are best placed to find a new job elsewhere may therefore have left the company before it closes, thus biasing the composition of the remaining labor force.
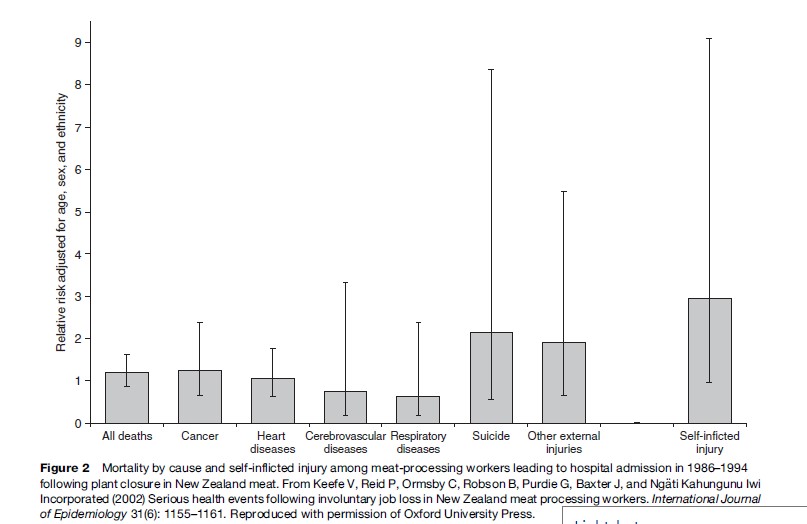
A good example of a closure study is that of a meat processing plant in New Zealand that closed in 1986 (Keefe et al., 2002; see Figure 2). A neighboring plant remained open until 1994, and the investigators were able to access hospital discharge and mortality data for both plants 9 years before and 8 years after the closure. Although this is by far the largest factory closure study to date, with nearly 2000 participants in both the study group and the control group, the number of deaths after 8 years was still relatively small, and none of the differences were statistically significant. However, those who were unemployed had an elevated suicide mortality (hazard ratio 2.15; 95% confidence interval 0.56–8.36). When combined with hospital admission after closure for nonfatal self-harm, this outcome was statistically significantly higher among those who had worked in the closed plant.
Unemployment
Mental Health
The effects of unemployment on different domains of mental health are by now well established. The most often studied outcomes are various self-reported measures of common mental disorders. For the effects to appear, long-term follow-up is not necessary, as the repercussions of unemployment can occur soon after unemployment has started and often before if the redundancy is preceded by a period of insecurity. Best evidence comes from factory closure studies and longitudinal studies that have followed participants into unemployment and/or reemployment.
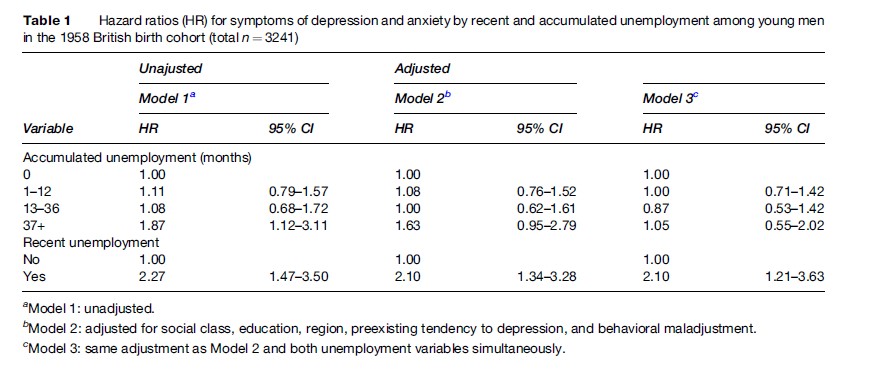
A study by Montgomery et al. (1999) of young men in the 1958 British birth cohort study is a good example (see Table 1). This study showed that, after adjusting for several socio-demographic characteristics and for the preexisting tendency to depression and behavioral maladjustment, both recent and accumulated unemployment were associated with symptoms of depression and anxiety that resulted in medical consultations. Further analyses showed that these associations were mainly driven by recent experience of unemployment. This and evidence from other studies indicate that unemployed persons adapt to unemployment and mental ill health stabilizes at an increased level after about 12 to 18 months. Furthermore, reemployment has been shown to reverse the effects of unemployment on mental health.
The mechanisms by which these effects occur are, to some extent, common sense; that is, deterioration and worry about one’s financial situation and the loss of self-esteem and loss of social support networks at work have an adverse effect on psychological well-being. Studies have shown that income change and borrowing after unemployment also explain an important part of increased mental health problems in unemployment. However, material explanations do not exclude more psychological explanations; for example, reemployment has been associated with improvements in mental health, regardless of financial circumstances.
Physical Morbidity And Mortality By Cause
Follow-up studies that have simultaneously assessed the effects of unemployment on mental health and physical health have usually found more consistent and larger effects on mental health than on physical health. In the majority of studies physical health has been measured by self-report of general physical health or symptom lists, but longitudinal evidence on the incidence of new disease is patchy. The most consistent evidence of the physical health effects of unemployment comes from studies of cause-specific mortality.
The association between unemployment and mortality has been well established in several longitudinal follow-up studies of individuals. The sizes of the effects vary widely, from an excess of 20–30% in England and Wales, to 60–70% in Denmark, to about 100% in Finland. These effects are strongest for mortality from suicide as well as accidents and violence. Considering the well-established effects of unemployment on mental health, this relationship seems plausible. The effects for other broad groups of causes of death are more varied, but excess mortality is observed at least for lung cancer and cardiovascular diseases. Only part of these associations can be explained by measured preexisting selection factors or mediating factors.

The effects of unemployment also appear to be associated more strongly with mortality among younger rather than older men and women and among those unemployed for extended periods of time. However, many of these study designs suffer from not being able to account for alternative explanations. The New Zealand factory closure study of meat-processing workers provides a cautionary finding; in this material an association between unemployment and suicide could be established (hazard ratio 2.15; 95% confidence interval 0.56–8.36), but unemployment was unrelated to other causes of death, as well as to hospital use for heart disease, cerebrovascular disease, cancer, and respiratory illness (Keefe et al., 2002).
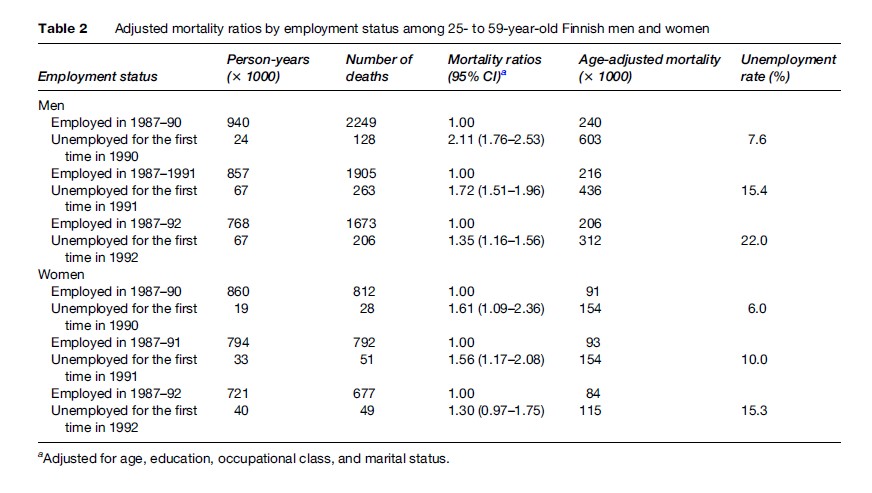
A similar cautionary note comes from analyses of the effects of unemployment on mortality at different levels of the national unemployment rate in Finland (see Table 2). At a time of low unemployment and strong demand for labor, those becoming unemployed may be more selected on the basis of their individual characteristics that are harmful to health. On the contrary, at a time of high unemployment, almost anyone can become unemployed; becoming redundant and/or remaining unemployed can be assumed to be less dependent on individual characteristics that increase the risk of ill health. Studies carried out in those circumstances may thus provide the best clue for the true causal effects of unemployment. The results to date show that the excess mortality of the unemployed is lower the higher the unemployment rate: those experiencing unemployment at low levels of unemployment have 111% excess mortality as compared to a 35% excess at the peak of the recession (Martikainen and Valkonen, 1996). This finding implies that selection may play a large role in explaining the association between unemployment and mortality. Similar results have been observed in Denmark.
Health Behaviors And Biomedical Risk Factors
One of the mechanisms by which unemployment may lead to deterioration in physical health (and also mental health) and may increase mortality is through change in health related behaviors and consequent changes in biomedical risk factors. Most longitudinal studies in this field relate the effects of unemployment to changes in tobacco smoking and alcohol use. However, the evidence that this causal pathway is implicated is contradictory, as both beneficial and adverse changes have been widely reported.
One of the reasons for the lack of a clear association may be the differential responses to the financial constraints of unemployment and changes in time use during unemployment. Although some unemployed individuals increase their participation in risky behavior, others may cut down on drinking and smoking to save money; still others may increase their level of physical activity as more time is available. It also appears possible that different subgroups of the unemployed react differently to changes in the availability of money and time and that these effects vary according to the duration of unemployment.
Research evidence that unemployment affects biomedical risk factors is more scarce even than the evidence on health-related behaviors. Increases in cholesterol levels, blood pressure, and immune reactions have been observed. However, most of these studies assess short-term changes, and it remains uncertain how important observed changes in the immune system are to the development of chronic disease.
Job Insecurity
As with unemployment, the strongest support for the causal precedence of job insecurity in the job insecurity–health relationship comes from studies of workplace closures and studies of changes in job security over time. Identifying those exposed to job insecurity is more difficult than identifying the unemployed, as no change in job status has occurred. Two approaches have produced fairly similar results. One approach presumes that those employed in a workplace that has been earmarked for closure or downsizing are exposed to job insecurity, although certain groups – for example, those very close to retirement and those who are confident about finding new work – may not feel at risk. The other approach ascertains those at risk by self-report. As for unemployment, most of the research to date has been conducted among employees accustomed to long-term secure employment and not among those workers for whom job insecurity is part of the psychological contract, such as those in seasonal employment.
Mental Health
Most studies that have examined the effects of job insecurity on health have looked at mental ill health as an outcome and often as the only outcome. Almost every study has documented consistent adverse effects on all measures of mental health, although a combined analysis of the association between job insecurity and mental health outcomes in 37 study samples has estimated the effect size to be medium rather than large, with a standardized effect of approximately 25% (i.e., an increase of one standard deviation in job insecurity score is associated with a 25% increase in mental health problems).
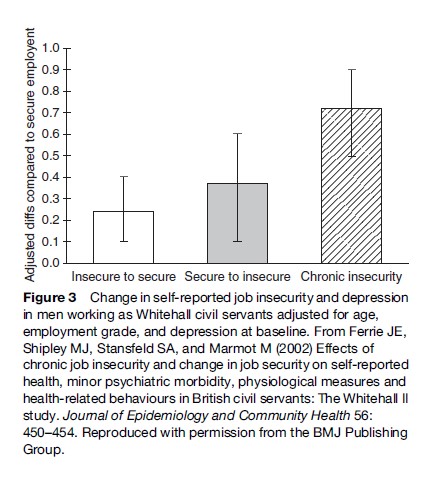
One study of change showed that, compared to employees who reported their jobs as secure at baseline and follow-up (2.5 years later), poor self-reported mental health was more prevalent among those who reported their jobs as secure at baseline but insecure at follow-up (Ferrie et al., 2002; see Figure 3). Among those who reported the reverse – that is, their jobs were insecure at baseline but secure by follow-up – a residual adverse effect on mental health was observed. However, those who reported exposure to job insecurity both at baseline and follow-up (chronic job insecurity) experienced the greatest prevalence of mental ill health.
Physical Health
As with the findings for unemployment, the body of evidence supporting an association between job insecurity and measures of physical health – general self-reported health measures, diseases, and premature mortality – is much smaller than that for mental health. Given the self-appraisal element in self-reported measures of general physical health, such as self-rated health over the last year, it is perhaps unsurprising that clear associations between job insecurity and self-reported physical health have been observed, although the evidence also shows that effects are independent of mental health. However, a meta-analysis of the association in 19 study samples assessed the standardized effect size of approximately 16% as small.
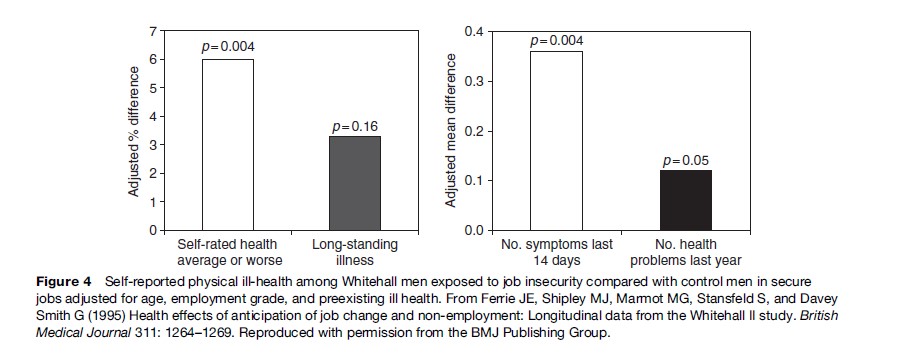
The Whitehall II study, a longitudinal study of white-collar civil servants, was able to examine the association between job insecurity and measures of general physical health under the conditions of a natural experiment (Ferrie et al., 1995, 2002). Well after the baseline data collection, one of the 20 departments participating in the study was sold to the private sector, a transfer of business in which the majority of the workforce lost their jobs. Increases were observed in nearly every measure of self-reported physical morbidity in both sexes three years prior to the sale when privatization was just a rumor. Increases were both relative to control employees in departments not facing privatization and, crucially, relative to preexisting physical ill health at baseline (see Figure 4).
These results have subsequently been confirmed in other analyses of data from the Whitehall II study, which examined job insecurity generated by organizational change across the British Civil Service. The results from both these studies confirm results from early, seminal work in this field among men in a factory manufacturing car paint and women and men employed in a meat processing plant in the United Kingdom.
Job insecurity has been shown to be associated with adverse changes in most biomedical risk factors that have been examined, but the effects are mostly nonsignificant. Although there is an indication that job insecurity is associated with an increase in heart disease, there is no evidence yet of an association between job insecurity and death from diseases or suicide. Job insecurity has also been shown to be associated with adverse effects on health outcomes of interest to the organization. For example there is some evidence of an increase in workplace injuries and accidents and reasonably good evidence that job insecurity is accompanied by an increase in self-certified and medically certified sickness absence. However, lower rates of sickness absence as well as sickness presenteeism (the tendency of people showing up at their work place despite ill health) among temporary workers and employees facing imminent threat of job loss have also been demonstrated.
As for unemployment, it has been proposed that the effect of job insecurity on physical health may be mediated via changes in health-related behaviors. However, there is little evidence to support or refute this hypothesis. Although some studies have found the effect of job insecurity on health to be partially explained by adverse changes in other characteristics of the work environment, such as job satisfaction, social support at work, and job control, much of the association between job insecurity and ill health remains unexplained and may be due either to direct effects of stress on the autoimmune system or unobserved health-related selection.
Implications
At present it is probably premature to evaluate the net consequences of recent labor market changes on health. The full impact of these changes brought about by technological change and deindustrialization has yet to be felt, and our current understanding of the labor market careers of individuals is far from perfect. It is premature to argue that all of the recent changes will have far-reaching detrimental effects. Although the proportion of ‘atypical’ employment contracts has increased, the financial burden of unemployment may have increased, and job insecurity is on the rise, the average length of tenure has not declined, and part-time and short-term contracts may in some circumstances be an avenue out of unemployment.
Furthermore, most of the research on the effects of unemployment has thus far examined only two states: unemployed vs. employed. Although relevant, evidence from such studies cannot be assumed to apply to situations in which atypical employment contracts are increasing rapidly. The emerging literature on job insecurity has broadened this picture. However, other forms of underemployment, involuntary part-time employment, and employment at wages below the poverty line are also the experience of working life for many employees, but less is known about their impact on health.
Research evidence on the health effects of unemployment and job insecurity is scarce in developing and newly industrialized countries, and the evidence gathered here has unknown relevance to employees in these countries. However, to the extent that unemployment, different forms of underemployment, and job insecurity lead to financial difficulties or worry and the loss of status and social networks, it is possible that their effects are more potent in societies where labor rights are more limited and social safety networks are less developed or nonexistent.
Summary
A full assessment of the nature of the relationship among unemployment, job insecurity, and health remains difficult to achieve. We have demonstrated the problems of causal inference with observational data in this area of public health and refer to some but by no means all of the best research evidence. We have focused our discussion on longitudinal analyses of change as these studies provide the best possibility to disentangle the complex web of causal pathways.
Whatever the explanation for the poor health of the unemployed, the true public health burden of economic recession, increasing unemployment, and job insecurity cannot be accurately estimated from the current research evidence. However, longitudinal follow-up studies of unemployment and reemployment have quite convincingly established their effects on various indicators of mental health, and a growing body of research on job insecurity provides similar evidence. Evidence on the effects of job insecurity and unemployment on physical health and mortality is more inconclusive; the nature and size of the effects remain difficult to determine. Conflicting reviews of scientific evidence on this topic in the past 20 years are a poignant reminder of this difficulty.
Bibliography:
- Ferrie JE, Shipley MJ, Marmot MG, Stansfeld S, and Davey Smith G (1995) Health effects of anticipation of job change and non-employment: Longitudinal data from the Whitehall II study. British Medical Journal 311: 1264–1269.
- Ferrie JE, Shipley MJ, Stansfeld SA, and Marmot M (2002) Effects of chronic job insecurity and change in job security on self-reported health, minor psychiatric morbidity, physiological measures and health-related behaviours in British civil servants: The Whitehall II study. Journal of Epidemiology and Community Health 56: 450–454.
- Keefe V, Reid P, Ormsby C, Robson B, Purdie G, Baxter J, and Ngati Kahungunu Iwi Incorporated (2002) Serious health events following involuntary job loss in New Zealand meat processing workers. International Journal of Epidemiology 31(6): 1155–1161.
- Martikainen P and Valkonen T (1996) Excess mortality of unemployed men and women during a period of rapidly increasing unemployment. Lancet 348: 208–213.
- Montgomery SM, Cook DG, Bartley MJ, and Wadsworth ME (1999) Unemployment pre-dates symptoms of depression and anxiety resulting in medical consultation in young men. International Journal of Epidemiology 28(1): 95–100.
- Bartley M and Ferrie JE (2001) Unemployment, job insecurity and health – Glossary. Journal of Epidemiology and Community Health 55: 776–781.
- Bartley M, Ferrie J, and Montgomery SM (2006) Health and labour market disadvantage: Unemployment, non-employment and job insecurity. In: Marmot M and Wilkinson RG (eds.) Social Determinants of Health, 2nd edn., pp. 78–96. New York: Oxford University Press.
- Dooley D, Fielding J, and Levi L (1996) Health and unemployment. Annual Review of Public Health 17: 449–465.
- Ferrie JE (2001) Is job insecurity harmful to health? Journal of the Royal Society of Medicine 94: 71–76.
- Ferrie JE, Marmot MG, Griffiths J, and Ziglio E (eds.) (1999) Labour market changes and job insecurity: A challenge for social welfare and health promotion. Report of the WHO, European Series, No. 81. Copenhagen, Denmark: World Health Organization.
- Hartley J, Jacobson D, Klandermans B, and Van Vuuren T (1991) Job Insecurity: Coping with Jobs at Risk. London: Sage Publications.
- Jin RL, Shah CP, and Svoboda TJ (1997) The impact of unemployment on health: A review of the evidence. Journal of Public Health Policy 18(3): 275–301.
- Kasl SV and Jones BA (2000) The impact of job loss and retirement on health. In: Berkman LF and Kawachi I (eds.) Social Epidemiology, pp. 118–136. New York: Oxford University Press.
- Mathers CD and Schofield DJ (1988) The health consequences of unemployment: The evidence. Medical Journal of Australia 168: 178–182.
- Quinlan M, Mayhew C, and Bohle E (2001) The global expansion of precarious employment, work disorganization, and consequences for occupational health: A review of recent research. International Journal of Health Services 31: 335–414.
- Shortt SED (1996) Is unemployment pathogenic? A review of current concepts with lessons for policy planners. International Journal of Health Services 26: 569–589.
- Smith R (1987) Unemployment and Health: A Disaster and a Challenge. Oxford, UK: Oxford University Press.
- Weber A and Lehnert G (1997) Unemployment and cardiovascular diseases: A causal relationship? International Archives of Occupational and Environmental Health 70(3): 153–160.
See also:
Free research papers are not written to satisfy your specific instructions. You can use our professional writing services to buy a custom research paper on any topic and get your high quality paper at affordable price.
ORDER HIGH QUALITY CUSTOM PAPER

Always on-time

Plagiarism-Free

100% Confidentiality



