
This sample Population and Labor Force Aging Research Paper is published for educational and informational purposes only. If you need help writing your assignment, please use our research paper writing service and buy a paper on any topic at affordable price. Also check our tips on how to write a research paper, see the lists of health research paper topics, and browse research paper examples.
Introduction
Aging, of both the general population of a country and specifically of its labor force, affects the economic growth rate and socioeconomic welfare and health status of both developed and developing countries. This is because the total economic productivity of a country is determined by three factors (Li and Me´rette, 2005) contributing to total economic production (as measured by gross domestic product [GDP]): (1) natural resources and capital input, (2) human resources or labor input, and (3) the technological base (total factor productivity) of the economy. This latter quantity might be empirically represented, for example, by the set of patents held by citizens of a country. The rate of generation of new technology (Manton et al., 2007) is a function of the level of scientific investment in research (especially in scientific manpower) and its productivity, and the efficacy of that investment will be affected by gains from prior research and redundancy in research. The latter affects the variety of new products produced and the emergence of new markets.
The primary issue we review in the following sections is the interaction of the three growth factors – capital, labor, and technology – in determining the rate of economic growth in the four ‘BRIC’ countries of Brazil, Russia, India, and China, which are hypothesized to grow more rapidly than other highly developed countries (e.g., the United States, Japan) and therefore dominate the global economy by 2050. Though technology affects the availability and productivity of capital inputs our review focuses more on human factors as they are modified by health-care inputs, technical training, and advances in biomedical research, which are all significantly altering the traditional relation of age to the level and duration of labor force productivity. We suggest that a currently undervalued, future avenue for national economic growth would be modifications of both aging and chronic disease processes by biomedical research and health-care system innovations. Indeed, this may require a reevaluation of human capital inputs into economic growth – especially of elderly persons.
Dramatic long-term changes in human productivity due to improved public health and nutrition were suggested by the work of Fogel and Costa on technophysiological evolution. With recent rapid improvements in public health, and health-care systems and technology, we argue that changes in human capital at later ages may accelerate in countries where large investments in the health of the elderly are now under way (e.g., Japan, United States, Western Europe [EU]). We feel the failure to aggressively address these issues in the BRIC countries could lead to a failure of the BRIC hypothesis (see section titled ‘The BRIC hypothesis about the role of developing countries in the global economy’). The necessity for considering the need for further biomedical research and improvements in the health care of older populations is driven both by population aging and the need for increasing years of educational and technical training for workers in modern technologically driven economies (e.g., Bell, 1974; Toossi, 2005).
What are interesting in the proposed analyses are changes in the relative balance of the three growth factors (labor, capital, technology) in determining the rate of economic growth in developed and developing countries. Specifically, some countries have recently grown rapidly because of the ready availability of natural resources, such as in Brazil and Russia, and some due to the availability of large amounts of inexpensive labor, such as in India and China. What are novel are views about the effects of technology on labor inputs at advanced ages (Murphy and Topel, 2006; Manton et al., 2007). In many models projections of economic growth are heavily dependent on the number of workers within an employable age range under extant conditions of health and occupation mix (e.g., ages 15–59). Increasingly, in developed countries, the effects of workers (labor inputs) on economic growth will need to be adjusted for qualitative factors affecting individual productivity at specific ages, such as training levels and age-related changes in population health and physical and cognitive function. Modern public health and health-care technology, at the least, can significantly extend the upper bound of the age range of the available labor force for many developed, and possibly in the future, developing countries. For example, in Britain there is consideration of raising the normal retirement age to 69 by 2050. In Japan it is argued that with an increase in the normal retirement age to 73.2 years having been proposed, retraining programs could target persons in their early 60s.
Thus it is now not sufficient in evaluating labor inputs to simply count the number of workers within a fixed age range, but to examine the level of health and training that dictate the productivity potential of each worker over a possibly widening age range where the mean age of the trained labor force is increasing. Some of this may be technological innovation described by total factor productivity but some will be reflected directly in intrinsic changes in the nature of human capital through interactions with environmental mechanisms like technophysiological evolution (Fogel, 2004).
This evaluation necessarily requires examining the effects of investment in biomedical research and healthcare innovations on labor productivity (Manton et al., 2007). Fogel and Costa (1997) have suggested that longer-term improvements in nutrition, health, and even enhancement of cognitive problem-solving skills due to techno-physiological evolution (Manton et al., 2006a, 2007) require a multidimensional quality ‘scale’ to weight each worker according to his or her productivity potential(s). Recent data suggest such effects on individual productivity due to health improvements at later ages have been growing at more rapid rates in the last 25 years in the United States and possibly other developed countries (Robine et al., 2003; Manton et al., 2006b).
These changes in the conceptualization of labor productivity will have effects on many health care and socioeconomic factors as well as on projections of the future rates of overall economic growth – and possibly of the stability of social and political infrastructures due to the resolution of social and medical problems inherent in the growth of older populations and workforces (Hall and Jones, 2007). To accomplish this, health-care and socioeconomic factors can be linked by the concepts of human capital at late ages and active life expectancy (Manton et al., 2006a, b) in models of the effects of research investment on economic growth (Murphy and Topel, 2006; Hall and Jones, 2007). That is, the economic consequences of population aging are modulated both by the average level of health status and functioning (physical and mental) maintained at specific older ages, as it affects labor force participation rates, individual productivity, and labor force growth and size. These effects also reflect the existing level of wealth in a society because, as disposable income for individuals increases, the value of an increment in health, and the relative level of expenditures on health care appropriate to achieve it, increases (Murphy and Topel, 2006). If functional status can be maintained to later ages then the ability to deal with population and labor force aging is enhanced because of the greater human capital and productivity maintained at older ages, and the level of long-term care (LTC) and other labor-intensive health services required to support chronically disabled elderly persons is reduced because of the growing effectiveness of medical care to reduce age-related functional impairments (Manton et al., 2007).
This suggests that increased investment (expenditures) in health care and biomedical research, despite arguments made in the United States and other countries, is often more than offset by increased human capital. That is, growth in health-care investment can be economically stimulating, with the degree of stimulation a function of the existing level of health and economic development, which leads to a growing economic value for each increment in health status (e.g., person-years lived, see Murphy and Topel, 2006). Thus, the better the average health status that is maintained at later ages in a particular country, and the greater its level of economic development, the greater the future share of GDP that should be invested in health care and research because of higher labor productivity and economic value resulting from the investment in human capital (Hall and Jones, 2007). This occurs because, as disposable income grows, the elasticity of health-care expenditures tends to be preserved while the elasticity for other consumer products decreases (Fogel, 2004). One of the factors we evaluate is the degree to which certain developing countries (i.e., BRIC), with their rapidly growing economies, may or may not be planning to systematically exploit health-care investment (including the areas of biomedical research and innovation) as a strategy to preserve growth momentum when their populations reach critical levels of population and labor force aging in the future.
In studying the effects of population and labor force aging as modulated by improvements of health among the elderly, one also has to be aware of the impact of these factors on the global economic competitiveness between countries at different levels of technological and economic development, degree of population aging, and of the effects of selective (at different skill levels) migration. We evaluate the implications of population and labor force aging for Brazil, Russia, India, and China and – to expand the range of conditions studied – include several additional former Soviet states and Asian countries currently experiencing population aging and rapid economic expansion. These countries are then compared with developed countries with generally more stable economic and social conditions ( Japan, the United States, EU) for their current and future positions in the global economic order.
Country Reviews
China
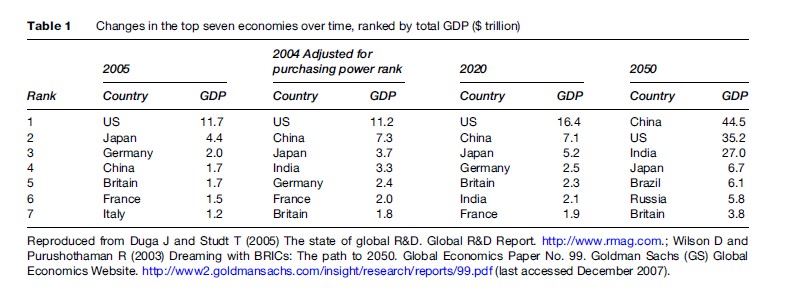
China is currently the country with the largest population in the world at 1.3 billion persons and the most rapidly growing economy. The Chinese GDP is expected to increase about 10% in 2007 (CIA Factbook, 2007) though GDP growth is eventually expected to taper to a more sustainable 5–6% in 10–15 years. Furthermore, although the nominal GDP of China currently appears relatively small compared to a number of other countries’ adjustments for purchasing power rank, equivalence suggests that its economy ($7.3 trillion) is already the second largest in the world (Table 1) (Duga and Studt, 2005). Indeed, recent CIA Factbook (2007) estimates suggest that in 2007 the Chinese economy ($10.2 trillion) was 78% of that of the United States ( $13.1 trillion).
A factor crucial to sustained socioeconomic development in China was the decision in 1979 to raise the average socioeconomic status of the Chinese population by reducing the fertility rate. Fertility rates were already falling (Hesketh et al., 2005) when the so-called one child–one family policy was initiated in 1979. From the 1950s to the 1970s the Chinese fertility rate declined from 5.9 to 2.9 (2.1 is considered the replacement level). The introduction of the new fertility policy – which, for example, limited births to one per couple in government worker and urban families but allowed two births for families in rural areas – further reduced the fertility rate from 2.9 to 1.7 (lower than the current fertility rate in the United States). The fertility rate was also below replacement levels for long-term population growth, which was to reduce the rate of growth of China’s population so that it was only 1.27 billion by the year 2000 (Congressional Budget Office [CBO], 2005) (Figure 2).
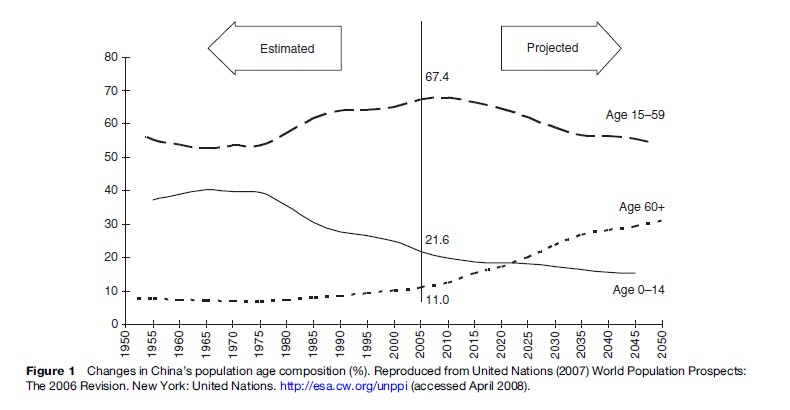
What is a surprise is that the Chinese population, due to this fertility policy, is currently one of the fastest aging populations in Asia. Asian countries are generally aging rapidly, with Japan having already reached a very high degree of population aging, and whose old age dependency rates are projected to surpass the United States in the next 30–50 years (CBO, 2005). This is caused not only by the rapid decline in the Chinese fertility rate but also by major improvements in mortality, for example, life expectancy increased over 20 years from 1950 to 1975 (CBO, 2005) (Figure 1). Currently, Chinese life expectancy is estimated to be 72.9 years (CIA Factbook, 2007).
What is also surprising is that Chinese fertility is tracking a similar temporal path to that experienced in Japan but with a 22–27-year lag. Japanese fertility rates dropped by half from 1947 to 1957 (Kuroda, 1987). In China, a similar decline in fertility (50%) occurred roughly 22 years later. As a consequence, the age distribution of the Chinese labor force (i.e., the population aged 15–59) will continue to improve between 2005 and 2015 and then will start to decay toward 2050 when 31.1% of the Chinese population is projected to be over age 60 (see Figure 1).
With the erosion of the ‘demographic’ dividend beginning around 2015 the era of exceptional Chinese economic growth that began in the 1970s will end so that ‘‘the next decade may be China’s last chance to join the ranks of developed countries’’ (Kwan, 2006: 3). Such problems will be exaggerated by limitations on natural resources and environmental quality in China – especially growing limitations on energy resources, increasing environmental damage, and the increased health-care demands of an aging labor force and elderly and oldest old population.
In 1982 the proportion of the Chinese population aged 65 and over was 5%. In 2005 the elderly population made up 7.5% of the total. In 2025 the proportion of elderly persons is projected to be 15%. Though lower than the current 20% elderly population in Japan today, which is projected to grow to 36% by 2050, there is the additional problem that 70% of Chinese elderly are still dependent on their offspring and family resources for health and LTC due to the current limitations of the pension and health-care systems in China. Only government officials and workers in large companies are adequately covered by pensions in China. This is referred as the ‘4:2:1’ problem, that is, that rapidly growing numbers of couples will be responsible for one child and four grandparents. The problem is particularly acute in rural areas where younger persons have tended to migrate from those areas to the growing labor markets in coastal urban areas. There is concern, however, about the effects of liberalizing the current fertility policy for fear that the Chinese population will significantly exceed the government’s population goal of 1.4 billion persons by 2010 and thereby compromise the current rapid economic growth rate.
One aspect of this growth that is unclear in China is in the trajectory of change in human capital in older workers. Two ways to increase human capital in an aging labor force involve making improvements in health and functioning at later ages, and increasing work skills by additional training. In terms of the technologically trained labor force, China, with 820 605 researchers, has a technical workforce second only in size to the United States (1.3 million researchers) (Duga and Studt, 2005).
China has illustrated their advantage over most developing countries in scientific training and research in producing almost 140 000 international patents from 2004 to 2006 (1 per 9285 persons) – still low compared to 595 000 in the United States (1 per 504 persons) over the same period. South Korea, despite its much smaller population size ( 49 million persons) has produced over 250 000 patents over those same 3 years (1 per 196 persons). By far the greatest producer (both relative to population and absolutely) of international patents is Japan with over a million (1 039 000) patents produced from 2004 to 2006 (1 per 122 persons) despite its relatively small (compared to China and India) declining and aging population. Thus, it could be argued that modest labor force aging, in part due to later ages at entry to the labor force (Toossi, 2005), may not be strongly detrimental to economic growth in highly developed, technologically advanced countries with advanced medical care systems. For example, policy makers in Japan appear less concerned about a decline from the population of 127 million persons in 2006 to roughly 110–100 million persons by 2050 than about maintaining the motivation of workers to be highly trained and to continue past, strong work ethics.
Technical innovation in advanced developed countries is thus clearly not a simple function of labor force or population size and raises questions about the nature of the continuance of rapid economic growth in China and India. It suggests, however, that the maintenance of the economic dominance of the United States, Japan, and the EU would have to come from much larger investments in scientific and biomedical research, growing investment in public health care, and improvements in each of their health-care systems. This would support rapid product obsolescence and short product half-lives and make it more difficult for China and India to make the necessary capital and research investments to support such rapidly evolving markets (Tolley et al., 2007). Indeed, it suggests that the United States, Japan, and the EU will rapidly have to make a transition to a postindustrial society (Bell, 1974), in which services and manual labor become relatively less important while scientific and professional manpower increases absolutely, and relatively, in value.
To achieve this the proportion of GDP invested in research in advanced economies will have to increase significantly from the 2–4% observed today. Specifically, in such economies the proportion of the economy dedicated to industries with intensive research needs (e.g., drugs and electronics) will increase as will the research needs for necessary technological advances of more mature industries (e.g., energy production and transportation). For pharmaceutical companies it is not uncommon to dedicate 12–18% of their revenues to research; for electronics and software the research investment might be 5–15% of company revenues (Duga and Studt, 2006). Thus, as such technology-intensive industries increase as a proportion of a country’s economy, one might easily see in the future the share of GDP dedicated to research increase in some countries to a range of 6–12%. This is easier to do in the mature economies in Japan and the United States, where the current proportion of economic output dedicated to maintain basic services and personal consumption is already much smaller than in China and India.
The problem for the United States is one of politics and policy: while research investment will grow in Asia (e.g., to 34.9% of the global research investment in 2005), it will decline 2% in the United States (from 32.7 to 31.9%) in the next 2 years. The EU, although it has not yet achieved its goal, intends to increase its share of GDP spent on research and development (R&D) to 3% – a higher rate than the United States, but in Europe’s larger overall economy (Duga and Studt, 2006).
China, in 2006, overtook Japan as having the second largest national expenditure on R&D ($136.3 billion vs. $127.8 billion). The rate of increase in R&D expenditures in China has averaged 17% per annum over the last 12 years – and 20% per annum in the last 5 years. This has tripled the share of GDP spent on research in China since 1995. This is 62% of the proportion of GDP spent on R&D in the United States in 2007 (1.6% vs. 2.6%) though the Chinese economy, according to a recent estimate, is growing almost four times (11.1%) as rapidly as the United States (Duga and Studt, 2006). The global share of R&D is increasing in China from 12.7% in 2005 to 14.8% in 2007 while the U.S. global share is declining. As suggested by differences in estimates of the purchasing power adjusted GDP (i.e., nearly $10 trillion for China in 2007 estimated in the CIA Factbook), it is possible that current international estimates of research spending in China are also too low. It is likely that the globalization of research will further increase that rate of growth as 61% of corporate survey responders (Duga and Studt, 2006) propose to invest in research facilities in China (62% would be doing so due to inexpensive labor; 40% due to Chinese government support of research).
Another fundamental issue is changes in the health of elderly and oldest-old individuals in China. It is difficult to get nationally representative health statistics for rural areas of China (Saito et al., 2003). The health-care system, along with economic activity, is strongest in large coastal cities. In rural, interior areas a heavy reliance is still placed on traditional medicine and the family, especially for the elderly. These demographic and human capital conditions raise questions about China’s economic future despite the recent large increases in GDP and financial reserves.
A critical problem then is how China will respond to demands for health care in the large and growing rural, elderly populations. Existing data suggest that elderly persons in China remain generally physically active (Saito et al., 2003). Life expectancy has been increasing but will the Chinese health-care system be able to respond to the growing LTC demands of its increasing elderly and oldest-old population while meeting the human capital and natural resource demands for its transition to a highly industrialized and technological state? A possible solution may be the recent interest in China in having it also dominate agricultural production as it has dominated certain types of manufacturing through its large human capital base. However, for this to occur, it will be even more crucial for China to deal with public health, human capital, and ecological issues in its interior rural areas that have experienced a major loss of younger workers ( 100 million) to coastal metropolitan areas.
It is thus a time of decision for those directing and controlling the Chinese economy. China’s current, huge foreign capital reserves ( $1.2 trillion) could be used to help capitalize a pension system for the 70% of the population (primarily rural) remaining uncovered, to modernize its health-care system for elderly and oldest old persons, and to expand its biomedical research base to help deal with the aging of its population and labor force. Specifically, the ability to ameliorate the consequences of chronic diseases like diabetes and cardiovascular disease at later ages could be promoted through public health measures and improvement in the health-care system, as has been done in the United States, Japan, and the EU. This could extend the working life span, particularly in the aging, rural population. The need for this is promoted by the recent, rapid emergence of chronic disease and disability in Asian populations – including China.
Alternatively, fiscal resources could continue to be used primarily to fund nonhuman capital economic expansion, for example, payment of rapidly increasing external energy prices (e.g., oil from Russia) or investment in alternative energy technologies (e.g., technical contracts with Russia for 75 new nuclear reactors). The choice between investment in human versus physical capital is complex, but one that has to be made soon for rapid Chinese economic growth to be sustained and to eventually make a transition to a postindustrial society (Bell, 1974).
India
India is the second of the currently emerging Asian economic giants. In contrast to China it has not instituted a nationwide fertility policy to restrict population growth. Its current fertility rate is about 3.4 compared to 1.7 in China. Thus the Indian population will continue to grow while the current Chinese rate of growth will, in the relatively near future, lead to slowing population growth (eventually even declines) and a shift to a much older population age distribution. India is thus projected to surpass China as the world’s most populous country by 2030 when they both reach 1.5 billion persons. Furthermore, because of the lack of a specific fertility policy there will be relatively more persons in economically productive ages in India than in China. Nonetheless, in large urban areas in India fertility rates have declined significantly. These declines are most evident in economically advantaged and highly educated families in large urban areas in the industrial south. Fertility rates remain high in rural areas in the north. This fertility gradient may also reflect the positive effects on individual productivity of smaller family size and improved child health and education (Fogel, 2004).
As a consequence, in India, like China, there will be considerable geographic heterogeneity within the country in the degree of population aging and economic growth – heterogeneity complicated because the areas with rapid population growth areas have populations that are relatively less well educated and trained. Thus, for the large Indian labor force to have the global economic impact projected for it by many analysts, considerable additional investment must be made in human capital. For example, only recently has the Indian government placed a strong emphasis on compulsory education for persons under 14 and to double Indian educational spending to 3% of GDP.
Lacking natural resources, full literacy, and with a large proportion of the population experiencing basic public health issues, for example, water and air quality (Rajan, 2006), there is a concern about whether recent, highly optimistic economic growth projections are realistic. A crucial factor in this regard is the proportion of the labor force that is highly trained. The indices for this are unclear in India. In 2004–06 India produced less than 3000 international patents, compared with 140 000 for China. In terms of numbers of researchers, India is also far behind China. With a population of a similar size, India only has roughly 130 000 researchers and 110 000 research technicians. Its global share of 4% of research is only 27% that of China, which is 14.8%. In India the government is taking the lead in funding science with 75% of research investment coming from government sources. One recent advantage for India is that like China, it is currently a major target of global research outsourcing because of inexpensive labor, especially in information technology (Duga and Studt, 2005).
Like China, a major concern for India is the lack of an effective government infrastructure for administering pensions, education, and public health. Most economic development is occurring in select major metropolitan areas. The potential for future social and political instability in India due to labor force and population aging is greater than in China.
The Russian Federation
The Russian Federation is extremely rich in natural resources. Indeed, the primary basis for the Russian Federation’s recent economic growth has been its large petrochemical reserves, their extraction and exportation, and recent increases in the price of oil and gas. Exports of oil and gas, particularly to Europe (and, in the future, possibly to China and India), have led to a very positive balance of payments which the current Russian government has used to build up their so-called economic stabilization fund. This fund, currently in its accumulation phase and given stability in oil pricing, is projected to become between 40–50% of its GDP by 2030 and could begin to approach the fiscal reserves accumulated by China due to influxes of ‘energy’ payments from Europe and, later, possibly China and India. Paradoxically, the burden of energy costs in China may be supported by cash influxes from the United States (there was a $232 billion balance of payment deficit with China in 2007).
Among the former Soviet states, the Russian Federation is the primary beneficiary of the oil and gas boom (World Bank, Moscow Office, 2006). A recent comparison of the Ukrainian and Russian economies, for example, showed their fundamental differences. While the Russian economy has been based on extractive industries, the Ukrainian (the second largest former Soviet state) economy was more heavily based on manufacturing and, indeed, showed immediately after the Soviet Union’s breakup initially) greater productivity increases than Russia. Only recently has Russian industrial productivity begun to increase faster than in the Ukraine.

Given the magnitude of natural resources in the Russian Federation it is surprising that the standard of living, and health status, of the majority of the Russian population has improved only slowly – if at all. Indeed, World Bank projections suggest that if life expectancy and health-care issues are not addressed in the next 20 to 30 years it could suppress, by 30%, the future growth of Russia’s GDP. It would appear that without intervention, a similar fate might afflict future Chinese economic growth.
This demographic labor force problem appears to be unrelated to literacy, which is almost 100% in the Russian Federation. The Russian Federation’s extremely strong technology training base was, until the breakup of the Soviet Union, primarily directed toward defense and military issues. Only recently has the Russian government decided to direct significantly more resources in research, which are economically valuable for the private sector (e.g., nanotechnology in areas such as biomedicine).
To illustrate, Russia received roughly 60 000 international patents from 2004–06, which places it 7th in the world (1 per 2333 persons) (Duga and Studt, 2005): investment in R&D is exploding in the post-Soviet era due to changes in the direction of government research funding. By emphasizing research, these statistics may understate Russia’s ability to grow economically in that much of the former Soviet Union’s investment in technology resided in its scientific human capital. There are 487 710 researchers and 330 614 technicians in a Russian population of 143 million people. This is behind only China and the United States in terms of absolute numbers, and exceeds even the United States on a population-adjusted basis. This is bolstered, for example, by Russian President Putin’s recent call to put to use whatever oil and gas revenues are necessary for Russia to rapidly dominate global nanotechnology for the future; these funding levels are even greater than for nuclear power.
Given the high level of technical training in the Russian population the demographic problems can be seen to reside not in training but in adverse changes in the health and life expectancy of the Russian population, especially for males. The Russian population is aging and declining in size, with very low birth rates and poor health. The net effect of these factors can be seen by the estimates of life expectancy and active/healthy life expectancy in Table 2.
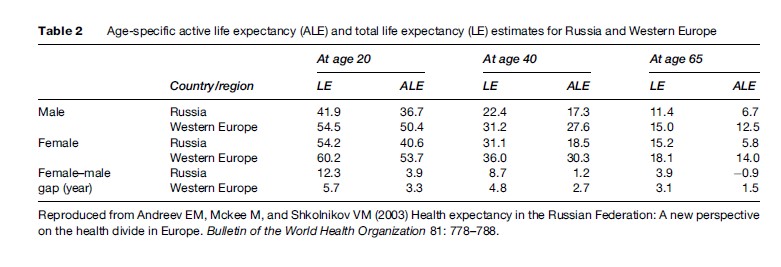
At age 20 the difference in survival between Russian and Western European males is large – 13.7 years (13.1 years for females) for active/healthy life expectancy and 12.6 years for total life expectancy. In one sense a low life expectancy limits the economic consequences of population aging by limiting the size of the elderly population. The adverse effects emerge in labor force aging by reducing the average number of work years for a population spending much of its early life in technical training.
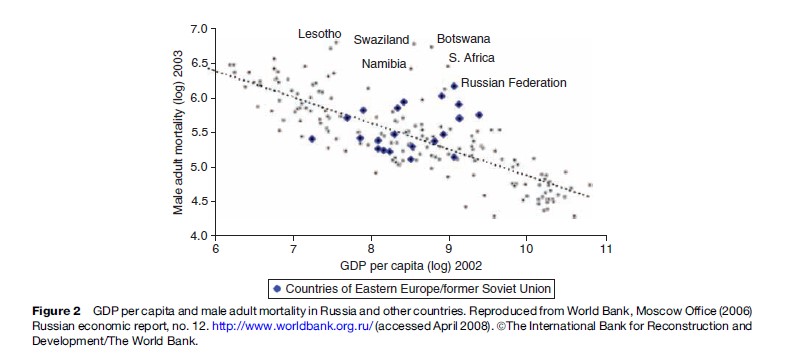
This is put in a broader perspective in Figure 2, in which mortality rates are plotted as a function of GDP per capita: as is clear, the Russian Federation has the highest male mortality rate of any former Eastern European/ Soviet state despite having close to the highest per capita GDP (in 2003). Its mortality rate is near the levels of select African nations, including several with much lower per capita GDPs (e.g., Lesotho, Swaziland, Namibia).
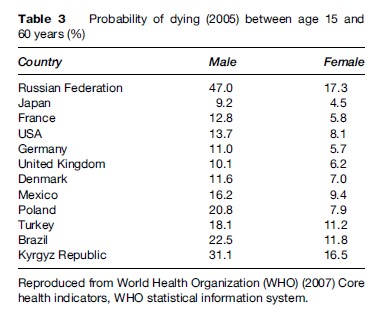
The causes of this poor health are currently not well known but, for males, smoking and alcohol consumption are leading candidates. In addition tuberculosis (particularly new, nonpulmonary types) is emerging in Russia and Eastern Europe, and HIV/AIDS (due to drug use) is growing rapidly. Indeed, the mortality rate of Russian males aged 15 to 60 significantly exceeds that of Turkey, Brazil, and even the Kyrgyz Republic – one of the least developed central Asian republics.
An examination of recent GDP growth in Baltic and Eastern European countries shows very rapid growth rates (6–10%) in 2006 (CIA Factbook, 2007). This suggests that the former Soviet economic system that broke up from 1989 to 1991 has reorganized on different principles and is attempting to regroup after the large declines in productivity that occurred immediately after the Soviet collapse. This rebound appears, in part, to be due to a redirection of production to commercial activities away from the prior focus on military uses. The reorganization is occurring most often in countries with low or negative population growth and raises the question of what levels of growth can be sustained as a new economic system emerges in Eastern Europe (Table 3).
Brazil
Brazil is demographically quite different from the Russian Federation. First, one natural resource it apparently does not have is extensive proven petrochemical and energy reserves except possibly for the development of ethanol and biofuels. Many of Brazil’s resources are agricultural and extractive (e.g., mining).
Second, its population is rapidly growing (currently about 190 million persons) in contrast to Russia. The groups that are most economically deprived are, surprisingly, the expanding, working-age population. The elderly, in contrast to India, China, and Russia, are relatively well provided for by Brazil’s current Social Security and pension systems. Additionally, the health and mortality of the elderly population has recently substantially improved. As in the three other countries of BRIC, there is considerable geographic heterogeneity in the well-being of the population, with health being considerably better in urban areas (Camarano, 2002).
As a generator of technological innovation Brazil is currently only a modest agent, producing only about 12 000 international patents between 2004 and 2006. As in India, much of the scientific research in Brazil is currently funded by the national government ( 60%). Brazil also currently has only a modest research workforce with 58 000 researchers and 23 000 technicians. A recent finding, however, involves increased research investment in information technologies (Duga and Studt, 2006). One of Brazil’s primary advantages is its ability to maintain an efficient and stable government infrastructure.
The BRIC Hypothesis About The Role Of Developing Countries In The Global Economy
The population dynamics of India and China, and the natural resource bases of Brazil and Russia, have led to the development of the BRIC hypothesis regarding country specific rates of growth in the global economy up to the year 2050. This hypothesis, promulgated in a Goldman-Sachs report in 2003 (DataMonitor, 2007), has since been elaborated on by other agencies including the World Bank.
The basis of the hypothesis is that the set of countries dominating the global economy will change dramatically by 2050, primarily due to the economic emergence of Brazil, Russia, India, and China. India and China will dominate globally because of their large human capital base and by heavily investing government resources in research. Indeed, their recent growth has reduced the global numbers of persons living in extreme poverty by 300 million (a reduction of 225 million in China alone) with much of the remaining, severely impoverished global population living in Africa. Although their human capital bases are much smaller than in China and India – and the quality of health in Russia is particularly suspect as a possible drag on economic growth – Russia and Brazil would have large natural resource bases. In the BRIC hypothesis, Europe and Japan (and later the United States) would lose their position in the global economy; their economies would continue to slowly increase by trading within that global economy whose growth would be stimulated by the BRIC countries. The projected increase for India, without a strong natural resource base, would be largely due to labor force demographics. Japan, in contrast, would be adversely affected by demographics in this model, with population declines starting in 2005 and 36% or more of its population over age 65 by 2050.
These changes in the global economy are projected by models of capital accumulation, productivity growth, and demographic transition, which are used to predict GDP growth (based on labor force growth, capital stock, technical progress, and changes in banking and trade). The effects of the projected changes in the global economy are presented in Table 1.
One intriguing country for comparison is the United States, which, in contrast to Japan, has a slowly growing population due to fertility near replacement levels and considerable in-migration. In addition, its existing labor force is highly technically trained and human capital at late ages, especially of those highly educated, is now being better preserved for economic roles (Manton et al., 2007). This is particularly important in that to develop a technologically advanced labor force, more persons aged 16–24 are remaining in school (Toossi, 2005, 2006). In addition, the capital base of the U.S. and Japanese economies are currently more technologically advanced leading to fewer ecological problems and a greater capacity to respond to energy resource problems – especially if China now has the expense of expanding its military presence in developing countries to maintain its access to external natural resources and energy. For China and India to advance as envisioned in the BRIC hypothesis considerable outsourcing of scientific research by the United States and EU will be necessary.
Factors probably not given adequate weight in the BRIC hypothesis are labor force training, environmental concerns, and population health issues, particularly at older ages. An extensive health-care infrastructure for the aging population does not exist in either China or India. Both China and India have growing ecological problems, particularly surrounding the availability of clean water. Finally, the existing physical infrastructure in both China and India needs considerable updating, especially in terms of energy sources and their ecological impact. Higher global prices for oil and gas would seem likely to reduce their growth rates in the near future. An additional issue is that while individual countries in Europe have medium to small economies, the size of the entire European economic system dominates even that of the United States. Thus, GDP growth for the EU could be much greater than projected on a country-by-country basis, particularly in terms of the growing impact and rate of technological innovation in future economic growth.
Pension, Health-Care, And Public Health Systems
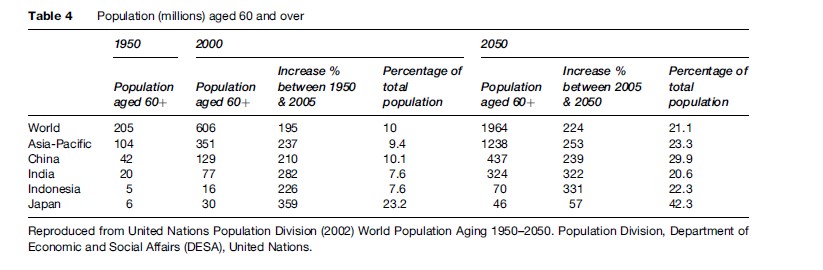
One of the factors affecting economic growth also apparently not well described in the BRIC hypothesis is the effect of population aging on pension systems and on providing health care to the elderly – particularly innovative health care to promote healthy aging, raise normal retirement age, and to help moderate pension demands. Table 4 gives United Nations (UN) statistics on Asian population aging, which illustrates population aging dynamics. The BRIC countries accounted for 41.5% of the world’s older population in 2000. The percent increase from 2000 to 2050 in China, India, and Indonesia far exceeds future increases in Japan. Additionally, the elderly population is itself aging with increases in the number of persons over age 80.
These population aging dynamics will have implications for specific health problems. For example, Brookmeyer et al. (2007) have recently projected rapid growth in the elderly population of those affected by Alzheimer’s disease. It is of interest that much of this growth is in Asian countries with large numbers of new cases emerging in China. Of possibly greater consequence is that Asian populations may have genetic predispositions to certain chronic diseases. Perhaps the greatest consequence is the rise of the prevalence of diabetes mellitus (type 2) in India, due both to dietary changes and genetic factors.

A broad prospective for this is provided in Table 5, which characterizes the speed of aging in north and central Asia. (In the rapid-aging group are Russia and four other Soviet Republics; predominantly Islamic republics show slower aging.) Table 6 shows the implicit pension debt (IPD) for selected countries, that is, the benefit promises a pension system makes to workers. IPD has grown rapidly with the proliferation of publicly managed, defined benefit pension plans during the twentieth century.
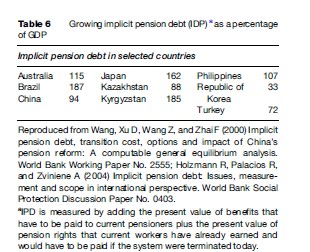
The IPD is large even in certain developing countries, such as Kyrgyzstan (Kyrgyz Republic) and the Philippines, where the population is still young (see Table 6). A similar pattern can be expected for other countries in the region as most countries have pay-as-you-go systems. The IPD becomes larger as the population ages. Rapid aging in Asia, as well as the dominance of publicly funded pension schemes, adds additional IPD burden with implications for future budget constraints. Pension liabilities can be overcome by one of three strategies: (1) reduce benefits or increase taxes, (2) increase total factor productivity, and (3) raise retirement ages (Li and Me´rette, 2005). Perhaps the most attractive options are the latter two, because they have benefits for human capital and the labor force. However, to carry out the latter two will require major reform of the LTC and health-care systems, which is particularly difficult in countries like India and China with their greater geographic and socioeconomic diversity.
Conclusion
This research paper examines possible changes in the global economic system due to the breakup of the Soviet economic system and the emergence of new economic powers, which are due to changes in the economic systems of several, large developing countries which have facilitated international trade so that they could more fully take advantage of their large, low-wage labor forces (e.g., India and China). Though several groups have forecast that the BRIC countries could begin to dominate the global economic order in the next 45 years, several factors may not have been adequately accounted for in those projections.
First, there is the effect of population aging that may turn the benefits of large labor forces, such as in China and India, into a growing liability beginning in 2010 and continuing to 2025. This problem will be enhanced by the current lack of adequate pension, social security, and health-care systems for the elderly in China, India, and Russia.
Second, the effects of population aging are amplified by limitations of health systems and public health issues. Specifically, the current populations in China and India are so large that the ability to support those populations when they become elderly is currently in question. In both China and India, only a select, well-educated, and highly trained portion of their populations, mostly living in large urban centers, is participating fully in the benefits of rapid economic growth. The total population in both China and India is quite heterogeneous with rural, less-educated populations growing more rapidly, implying that a lopsided internal economic development process exists in those countries, which could contribute to future social, economic, and political instability.
In the United States, and especially Japan, despite much smaller populations there has been more rapid technological development due to greater past investment in scientific research. It is currently unclear if China and India will have sufficiently rapid technological development to modernize their infrastructure quickly enough to deal with both the effects of rising energy costs and the emerging effects of labor force aging. In this view it is crucial to see how human capital at late ages may be increased by improved investment in health-care services and biomedical research.
Third, the economic models used to project the growth of the BRIC countries may not have adequately reflected the growth-retarding effects of a number of ecological factors – particularly the availability of adequate clean water sources.
Fourth, the models appear not to explicitly reflect future energy technology, particularly the use of nuclear fuels. The natural reserves of nuclear fuels have an entirely different geographic distribution, and set of economic implications, than petrochemicals (e.g., Australia, Canada, and Kazakhstan currently have the largest known reserves of uranium).
Fifth, the model seems not to acknowledge the possible effects of economic restructuring of both Western and Eastern Europe, which could form the future dominant economic system.
Sixth, a new stage of economic development may emerge in Europe, Japan, and the United States that is stimulated by past accumulated investments in research and will lead to new economic structures in which investment in research as a portion of GDP is several-fold higher than today (Manton et al., 2007) to produce a broader and faster rate of technological innovations.
As a consequence it appears that for the BRIC hypothesis to be true, there is a relatively narrow temporal window for China and India to dominate the global economic order due to the inevitable consequences of population aging, increases in health service demands, energy costs, and ecological factors on their future rates of economic growth. In both countries more resources would have to be directed into the health care for elderly persons to enhance human capital. In Russia, the scale of the population health problems is quantitatively much smaller, but is currently qualitatively more serious – both for overall population health and future economic growth.
Bibliography:
- Andreev EM, Mckee M, and Shkolnikov VM (2003) Health expectancy in the Russian Federation: A new perspective on the health divide in Europe. Bulletin of the World Health Organization 81: 778–788.
- Bell D (1974) The Coming of Post-Industrial Society. New York: Harper Colophon Books.
- Brookmeyer R, Johnson E, Ziegler-Graham K, and Arrighi HM (2007) Forecasting the global burden of Alzheimer’s disease. Alzheimer’s and Dementia 3: 186–191.
- Camarano AA (2002) Brazilian populating ageing: Differences in well-being by rural and urban areas. Second UN World Assembly on Aging. Rio de Janeiro: Instituto de Pesquisa Econoˆ mica Aplicada.
- Central Intelligence Agency (CIA) (2007) CIA World Factbook 2007. Washington, DC: CIA. https://www.cia.gov/library/publications/the-world-factbook (accessed December 2007).
- Congressional Budget Office (CBO) (2005) Global population aging in the 21st century and its economic implications. Washington, DC: The Congress of the United States.
- DataMonitor (2007) Key growth markets: Opportunities and challenges in Brazil, Russia, India and China. http://www.datamonitor.com/ industries/research/?pid=DMCO0338&type=Report (accessed December 2007).
- Duga J and Studt T (2005) The state of global R&D. Global R&D Report. http://www.rdmag.com.
- Duga J and Studt T (2006) Globalization alters traditional R&D rules. Global R&D Report 2007. http://www.rdmag.com.
- Fogel RW (2004) The Escape from Hunger and Premature Death, 1700–2100: Europe, America and the Third World. Cambridge, UK: Cambridge University Press.
- Fogel RW and Costa DL (1997) A theory of technophysio evolution, with some implications for forecasting population, health care costs, and pension costs. Demography 34(1): 49–66.
- Hall RE and Jones CI (2007) The value of life and the rise in health spending. Quarterly Journal of Economics 122: 39–72.
- Hesketh T, Lu L, and Xing ZW (2005) The effect of China’s one-child family policy after 25 years. New England Journal of Medicine 353: 1171–1176.
- Holzmann R, Palacios R, and Zviniene A (2004) Implicit pension debt: Issues, measurement and scope in international perspective. World Bank Social Protection Discussion Paper No. 0403. Washington DC: The World Bank.
- Kuroda T (1987) Population aging in Japan, with reference to China. Asia-Pacific Population Journal 2(3): 3–22.
- Kwan CH (2006) China in transition: China facing the challenge of aging population. Research Institute of Economy, Trade and Industry (RIETI). http://www.rieti.go.jp/en/china/06112801.html (accessed December 2007).
- Li H and Me´ rette M (2005) Population ageing and pension system reform in China: A computable overlapping-generations general equilibrium model analysis. Journal of Chinese Economic and Business Studies 3: 263–277.
- Manton KG, Gu X, and Lamb VL (2006a) Change in chronic disability 1982 to 2004–2005: Long-term changes in function and health in the U.S. elderly population. Proceedings of the National Academy of Sciences 103: 18374–18379.
- Manton KG, Gu X, and Lamb VL (2006b) Long term trends in life expectancy and active life expectancy in the United States. Population and Development Review 32(1): 81–105.
- Manton KG, Lowrimore G, Ullian A, Gu X, and Tolley HD (2007) Labor force participation and human capital increases in an aging population: Effects on national investment in research. Proceedings of the National Academy of Sciences 104: 10802–10807.
- Murphy KM and Topel RH (2006) The value of health and longevity. Journal of Political Economy 114: 871–904.
- Rajan SI (2006) Population ageing and health in India. Mumbai, India: The Centre for Enquiry into Health and Allied Themes (CEHAT).
- Robine JM, Romieu I, and Michel JP (2003) Trends in health expectancies. In: Robine JM, Jagger C, Mathers CD, Crimmins EM, and Suzman RM (eds.) Determining Health Expectancies, pp. 75–101. West Sussex, UK: Wiley
- Saito Y, Qiao X, and Jitapunkul S (2003) Health expectancy in Asian countries. In: Robine JM, Jagger C, Mathers CD, Crimmins EM, and Suzman RM (eds.) Determining Health Expectancies, pp. 289–318. West Sussex, UK: Wiley
- Tolley DH, Palmar H, and Stewart T (2007) The Cost of New Technology in Health Care. Working paper.
- Toossi M (2005) Labor force projections to 2014: Retiring boomers. Monthly Labor Review 128(11): 25–44.
- Toossi M (2006) A new look at long-term labor force projections to 2050. Monthly Labor Review 129(11): 19–39.
- United Nations (2007) World Population Prospects: The 2006 Revision. New York: United Nations. http://esa.cw.org/unppi (accessed April 2008).
- United Nations Population Division (2002) World Population Aging 1950–2050. Population Division, Department of Economic, and Social Affairs (DESA), United Nations. New York: United Nations. http://www.un.org/pubs/ (accessed April 2008).
- Wangy, Xu D, Wang Z, and Zhai F (2000) Implicit pension debt, transition cost, options and impact of China’s pension reform: A computable general equilibrium analysis. World Bank Working Paper No. 2555. http://ideas.repec.org/p/wbk/wbrwps/2555.html (accessed April 2008).
- Wilson D and Purushothaman R (2003) Dreaming with BRICs: The path to 2050. Global Economics Paper No. 99. Goldman Sachs (GS) Global Economics Website. http://www2.goldmansachs.com/ insight/research/reports/99.pdf (accessed December 2007).
- World Bank, Moscow Office (2006) Russian economic report, no. 12. http://www.worldbank.org.ru/ (accessed April 2008).
- World Health Organization (WHO) (2007) Core health indicatiors, WHO statistical information system. http://www.who.int/whosis/database/core/core_select.cfm (accessed April 2008).
- Copeland C (2007) Labor force participation: The population age 55 and older, Employee Benefit Research Institute. EBRI Notes 28(6): 2–9.
- World Bank (2003) World Development Indicators 2003. Washington, DC: World Bank.
See also:
Free research papers are not written to satisfy your specific instructions. You can use our professional writing services to buy a custom research paper on any topic and get your high quality paper at affordable price.
ORDER HIGH QUALITY CUSTOM PAPER

Always on-time

Plagiarism-Free

100% Confidentiality



